Download
1 / 61
610 likes | 782 Views
Selektive TNF ï¡ -Blockade durch Remicade (Infliximab) bei Patienten mit Morbus Crohn. Die Wunderwaffe ?. Morbus Crohn. Problem

E N D
Selektive TNF-Blockade durch Remicade (Infliximab)bei Patienten mit Morbus Crohn Die Wunderwaffe ?
Morbus Crohn Problem • Schwerwiegende klinische Symptome: Diarrhoe, abdominale Schmerzen, Fieber, Gewichtsverlust, Fistelbildung, extraintestinale Manifestationen, chronischer Verlauf mit transmuraler Entzündung Lokalisation im gesamten Gastrointestinaltrakt möglich • Standardtherapie mit Steroiden, Aminosalicylaten und Immunsuppressiva (Azathioprin, Methotrexat, Ciclosporin): oft unzureichend effektiv und mit Nebenwirkungen behaftet
Pathogenese der chronischen Entzündung bei Morbus Crohn Ein Ungleichgewicht zwischen pro- und antiinflammatorischen Zytokinen in der Darmmukosa verursacht chronische Entzündungsreaktionen.
Schlüsselfunktionen von TNF proinflammatorische ZytokineChemokine verstärkte Entzündungs-reaktion Makrophagen Endothel(Blutgefäße) Fibroblasten Darm-Epithel vermehrte Zellinfiltration Adhäsionsmoleküle TNFa akute-Phase-Reaktion CRP-Anstieg im Serum Synthese von MetalloproteinasenKollagenproduktion Gewebeumbau IonentransportPermeabilität gestörte Barriere-funktion
Aufbau von Infliximab Humane konstanteRegionen Murine variable Regionen (Bindung an TNFa) • monoklonaler chimärer IgG1-Antikörper • bindet mit hoher Affinität und Spezifität an TNF Knight JM, et al. Molecular Immunology. 1993; 16:1443-53.
Makrophage oder aktivierte T-Zelle TNFa TNF-Rezeptor Zielzelle Infliximab Neutralisation von TNF durch Infliximab van Deventer S. Gut. 1997; 40:443-48. Scallon BJ. Cytokine. 1995; 7:251-59. Feldman M., et al. Advances in Immunology. 1997; 64:283-350.
Studiendesign • doppelblinde, randomisierte, placebokontrollierte Multizenterstudie • 108 Patienten mit einer Krankheitsdauer 6 Monate • CDAI zwischen 220 und 400 Punkten • Begleitmedikation: Aminosalicylate beliebige stabile Dosis Prednison 40 mg / Tag Azathioprin / 6-MP beliebige stabile Dosis Targan S, et al. NEJM. 1997; 337:1029-35.
Klinische Remission (CDAI 150 Punkte) Remission (%)nach 4 Wochen 1/24 7/28 p-Wert vs. Placebo Targan S, et al. NEJM. 1997; 337:1029-35.
Klinisches Ansprechen (CDAI-Reduktion ³ 70 Punkte nach 4 Wochen) klinisches Ansprechen nach 4 Wochen (%) 4/24 18/28 p-Wert vs Placebo Targan S, et al. NEJM. 1997; 337:1029-35.
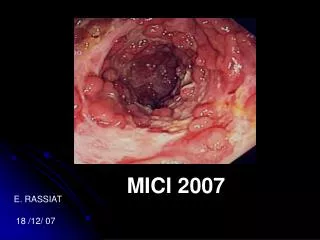
Endoskopischer Befund vor Behandlung 4 Wochen nach Behandlung van Dullemen HM, et al. Gastroenterology. 1995; 109:129-35.
Histologischer Befund (HE-Färbung) vor Behandlung 4 Wochen nach Behandlung
Fallbeispiel einer abdominalen Fistel Vor Behandlung nach2 Wochen nach 10 Wochen nach 18 Wochen Present D, et al. NEJM. 1999; 340:1398-405.
Kontrolluntersuchung nach 4 Wochen bei allen Kontrolluntersuchungen innerhalb von 8 Wochen 100% 100% 100 100 90% 86% 80 80 67% 65% 57% Ansprechrate (%) 60 60 50% 40 40 20 20 4/6 7/7 8/8 19/21 3/6 6/7 4/7 13/20 0 0 1mg/kg 5mg/kg 10mg/kg allePatienten 1mg/kg 5mg/kg 10mg/kg allePatienten Infliximab Infliximab Klinisches Ansprechen von Infliximab bei Kindern
Zusammenfassung (Kinder) • Pharmakokinetik von Erwachsenen und Kindern ist vergleichbar • nach 4 Wochen zeigten 65 % der Patienten ein klinisches Ansprechen und 25 % kamen in Remission • eine endoskopische Verbesserung konnte beobachtet werden • gute Verträglichkeit: keine schwerwiegenden Infusionsreaktionen, keine Antikörper gegen Infliximab oder Antikörper gegen ds-DNS • Infliximab zeigt einen sehr guten Therapieerfolg bei therapie-refraktärem Morbus Crohn im Kindesalter
Sicherheitsdaten von Infliximab • Infusionsdauer mind. 2 Stunden, Nachbeobachtungszeit 1 Stunde • gelegentlich traten Infusionsreaktionen auf (Symptome wie z.B. Hitzegefühl, Kopfschmerzen, Hautrötungen, Juckreiz, Übelkeit) • durch Verlangsamung bzw. Unterbrechung der Infusion oder evtl. Gabe von Antihista-minika/Kortikosteroiden kam es schnell zum Rückgang der Symptomatik
Häufigste Nebenwirkungen Angaben aus klinischen Studien bei Morbus Crohn und rheumatoider Arthritis Placebo Infliximab Kopfschmerzen 13% 21% Infektionen der oberen Atemwege 12% 16% Übelkeit 13% 15% Husten 3.1% 8.8% abdominale Schmerzen 5.7% 8.7%
Infektionen • bei jeweils 5 % der mit Infliximab behandelten Patienten und der Placebo-Patienten traten schwere Infektionen (wie z.B. Pneumonie) auf • die Infektionen waren durch entsprechende Medikation gut therapierbar • ein erhöhtes Infektionsrisiko ist für diese Patientengruppen aufgrund der Grunderkrankungen und der immunsuppressiven Begleittherapien bekannt
Subjektive Einschätzung O., Marcus: Beschwerdefreiheit ca.2 Tage nach Infusion - kann wieder durchschlafen - hat erstmals Hunger / Appetit - neuer Lebensmut Vater: - Verhalten des Sohnes sehr positiv verändert - hat wieder Lust zum Fahrradfahren - hat keine Depressionen mehr
Subjektive Einschätzung G., Kenneth: „Nach Infusion geht es mir sehr gut“ - Stuhl geform, kein Blut, kein Schleim - erstmals wieder Durchschlafen möglich - Bauchschmerzen „wie weggeblasen“ - gute Laune Eltern: - zunächst (nach ersten 3 Infusionen) sehr zufrieden - positiver Effekt hält ca. 3 Wochen an, immer kürzere Wirkungsdauer
Subjektive Einschätzung J., Juliane: Nach Infusion Wohlbefinden - glaubt, nur mit Remicade-Theapie ihre Berufsausbildung durchstehen zu können „Remicade-Sucht“ Mutter: - möchte Therapie auch nach Vollendung des 18.Lebensjahres fortführen Problem: Wirkung hält nur ca. 4 Wochen an, danach Bauchschmerzen, kein Appetit, Depression
Fisteln G., Anja + T., Rene -
Zusammenfassung • Infliximab (Dosis 5 mg/kg) führte zu einer schnellen Besserung der Morbus Crohn Symptome • klinisches Ansprechen war im Gegensatz zur Studie bei den eigenen Patienten nicht eindeutig assoziiert mit endoskopisch sichtbarer Mukosaheilung, bzw. histologischer Besserung • der Therapieerfolg hielt bei der Studie durchschnittlich 2-3 Monate, bei den eigenen Patienten 4 Wochen an • Vorsicht !
Adacolumn Apheresis System Flow rate: 30mL/minute Apheresis time: 60 minutes Total apheresis volume:1800mL P Adacolumn Vein Blood return Blood draw Vein Anticoagulant port
Legal Status • Adacolumn is indicated • for induction of remission in patients suffering from active Ulcerative Colitis • for the treatment of objective and subjective symptoms in patients suffering from active Rheumatoid Arthritis not responding to standard therapy • Adacolumn is approved and reimbursable in Japan • Adacolumn is CE-certified by the „TÜV“
dacolumn Granulocyte and Monocyte Apheresis Therapy Carrier Cellulose acetate beads Carrier weight 220g Main Body Polycarbonate Size 60mmØ ×206mm Filling solution Physiological saline Column void volume 130mL Sterilization method Autoclave at high vapor pressure
Tokyo Tokyo Women's Medical University Tokyo University International Medical Center of Japan Odate Municipal Hospital Hirosaki University Niigata University Hyogo College of Medicine Gunma University Tohoku University Fukushima Medical University Jichi Medical School Chiba University Hamamatsu University School of Medicine Oita Medical University Adacolumn Clinical Study Sites(14 Institutions)
Summary of Adacolumn Clinical Study Protocol in Patients with Active Ulcerative Colitis Primary endpoint: To assess and evaluate the safety and efficacy of Adacolumn, patients with Ulcerative Colitis using Adacolumn were compared to patients treated with conventional drugs Parallel controlled trial with 120 patients Adacolumn apheresis: 60 patients Conventional drugs: 60 patients Prednisolon, 5-ASA, SASP Shimoyama, T.; J. Clin. Apheresis 18:117-131, 1999
Clinical Efficacy - Ulcerative Colitis • Multicenter randomized comparative trial of standard therapy and of therapy with Adacolumn • 14 centers in Japan • 105 patients were enrolled and randomized whereas 53 patients received Adacolumn and 52 patients received standard therapy according to the guidelines of the national Japanese Ministry of Health • Diagnoses were performed using clinical symptoms, endoscopy, histology and X-rays Shimoyama, T.; J. Clin. Apheresis 18:117-131, 1999
Clinical Efficacy - Ulcerative Colitis • Standard therapy consisted of prednisolone, salazosulphapyridine and 5-amino-salicylic acid • Adacolumn apheresis 1x weekly for 5 weeks • Patient age: 12-76 Years • Exclusion criteria: Pregnancy/lactation, systolic blood pressure 80 mm Hg, anemia with < 8 g/dL Hb, increased tendency for coagulation • Degree of the severity was classified using stool frequency, macroscopic visible blood in stool, fever, tachycardia (frequency 90), hemoglobin level and ESR (rate 30 mm) Shimoyama, T.; J. Clin. Apheresis 18:117-131, 1999
Adacolumn Clinical Study Protocol in Patients with Ulcerative Colitis (UC) Conventional Drugs* Adacolumn (1 apheresis/wk × 5 wks) -2 1 2 3 4 5 6 7 Time (week) Overall assessment *Expert Committee on IBD, the Ministry of Health and Welfare of Japan Shimoyama, T.; J. Clin. Apheresis 16:1-9, 2001
Clinical Efficacy - Ulcerative Colitis Baseline after Adacolum apheresis Baseline after Adacolum apheresis 7,8 8 90 84,9 7 80 70 6 60 4,9 5 Frequency (%) 50 Patients (%) 4 38,5 40 3 30 2 20 10 1 0 0 Blood in stool (macrosc. visible) Mean frequency of stool (p < 0.001) (p < 0.001) Shimoyama, T.; J. Clin. Apheresis 18:117-131, 1999
Adverse Reactions Adacolumn Drugs Therapy Total 8 40 1 1 1 • Headache • Dizziness on standing • Dizziness Circulatory and respiratory organs 1 • Nausea • Duodenal perforation Digestive organs 1 • Fever • Flushing 2 2 Hypersensitivity • Liver disorder (mild) • Liver disorder 4 2 Liver disorder Shimoyama, T.; J. Clin. Apheresis 18:117-131, 1999
Adverse Reactions II Adacolumn Drugs Therapy • Osteoporosis • Reduced bone mass • Compressed fracture of lumber vertebra 3 3 Musculoskeletal symptoms 2 Lipid and protein metabolism disorders • Moon face • Hypoproteinaemia • Hypercholesterolaemia 10 2 1 Dermatological disorders • Acne • Pyoderma gangrenosum 5 1 Others 6 Shimoyama, T.; J. Clin. Apheresis 18:117-131, 1999
Adacolumn Summary Indication: Adacolumn is indicated for the treatment of UC (and potential other autoimmune diseases which are under investigation) Pathophysiology: 1) Reduction of granulocytes and monocytes 2) Changes of granulocyte adhesion Clinical findings: 1) Remission and improvement of clinical symptoms 2) Superiority vs. standard therapy - especially in severely affected patients 3) Reduction of steroid doses Tolerability: 1) Superior to standard therapy (less and milder side-effects)
Pyoderma Gangrenosum(UC) 38 year old male. Duration of disease = 3 years. Before treatment After 5th treatment T. Kanekura, et. al., J. American Academy of Dermatology (2002 in press)