ETATS DE CHOC
ETATS DE CHOC. Dr.Carvalho Martin Endocrinologue- Médecine Urgence. DEFINITIONS-GENERALITES. URGENCE VITALE I.Circulatoire →Hypoxie Tissulaire Choc Cardiogénique /Hémorragique Choc Anaphylactique / Septique TTT: O2, Rx Vasculaire,Drugs. Inotropes TTT Etiologique MAUVAIS PRONOSTIC.

ETATS DE CHOC
E N D
Presentation Transcript
ETATS DE CHOC Dr.Carvalho Martin Endocrinologue- Médecine Urgence
DEFINITIONS-GENERALITES • URGENCE VITALE • I.Circulatoire→Hypoxie Tissulaire • Choc Cardiogénique /Hémorragique • Choc Anaphylactique / Septique • TTT: O2, Rx Vasculaire,Drugs. Inotropes • TTT Etiologique • MAUVAIS PRONOSTIC
CAUSES-PHYSIOPATHOLOGIES • Choc Cardiogénique:↓D.C→↓Perf. Tissul. • Causes: -↓Contraction Myocardique: IDM,drugs, Cardiopathie dilatée hypokinétique • Troubles du rythme:TSV,BSinoA, BAV • Pathologies valvulaires et Prothétiques • Dysfonction du VD: Tamponnade,E.Pulmonaire.Infarct du VD
CAUSES-PHYSIOPATHOLOGIES • Choc Hémorragique:↓++de sang→anémie • Les 2 mécanismes→Hypoxie Tissulaire • Saignements internes ou externes; • Hgies Digestives-Pelviennes • Trauma:Hémothorax-hémopéritoine-hématome profond( Rate, Foie,Psoas, Rétropéritonéal)
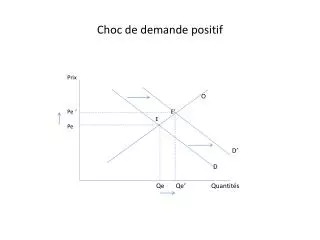
CAUSES-PHYSIOPATHOLOGIES • Choc Anaphylactique:Réaction après contact avec un allergène • Libération de médiateurs vasoplégiants→ • ↓RVS et ↑Perméabilité capillaire • 1er temps:↑DC par ↑F.C→PA stable • 2ème temps:Choc ↓avec D.C et donc P.A↓ • Causes:curares,ANTB,Prod.Iodés,insecte.
CAUSES-PHYSIOPATHOLOGIES • Choc Septique: • Anom.Cardio-vasculaires→O2 mal distribué en réponse inflammatoire à l’action des bactéries. • Phase Hyperkinétique: -↑D.Ccompensant↓RVS • Phase Hypokinétique: -↓D.C par acton des médiateurs de l’inflammation. • Causes: -pneumopathie, pyélonéphrite,cholecystite
DIAGNOSTIC CLINIQUE • Diminution de La P.A (PAS <80mm Hg) • FC augmente : pouls filant • Oligoanurie (< 30ml/h) • Neuro:confusion, désorientation,agitation • Respiratoires:polypnée ou cyanose • Cutanés:Marbrures,extrém.froides,sueurs. • Recherche d’étiologie
DIAGNOSTIC CLINIQUE • Recherche Etiologique • Septique:fièvre,frissons,hypothermie, signes infectieux focalisés • Hémorragique:paleur, hémorr.extériorisée • Cardiogénique:I.cardiaquegauche et Dte. • Anaphylactique:dyspnée laryngée,oedème de quincke, rash, nausées.
DIAGNOSTIC PARACLINIQUE • Gazométrie:Acidose métabolique • Iono sang:I.R. fonctionnelle(rein de choc) • Bilan hépatique: Foie de choc • NFS:anémie,↑GB,neutropénie,↓Plaquettes • Recherche de CIVD;Coag perturbé • Enzymes cardiaques:CPK, tropo, • Dosage CRP,Test de thorn. • Bilan infectieux • ECG, Rx Thorax, Echo Coeur, Cathé coeur
EVOLUTION • Syndrome de Défaillance multiviscérale 1/ Atteinte Rénale 2/ Atteinte Hépatique 3/ Atteinte Hématologique: CIVD 4/ Complications du décubitus: -escarres (Soins quotidiens) -Thromboses veineuses et E.P 5/Complic cathéters et sondes:Lymphangites
TRAITEMENT • Prise en Charge initiale: Rôle Infirmier+++ 1/ Oxygénothérapie 2/ VVP(2)ou VVC (intérêts) 3/Cathéter Radial,huméral,autre(intérêts) 4/Ventilation assistée (VNI ou intubation) 5/ Constantes:TA,FC, PVC,T°,Spo2 6/Surveillance clinique:agitation, marbrures, sueurs, etc… 7/ Bilan paraclinique:Gazo,iono, NFS,enzymes cardiaques et hépatiques,bilan infectieux.
TRAITEMENT • Choc Cardiogénique:Etiologique -1/Angioplastie si IDM -2/Fibrinolyse ou embolectomie si E.Pulm. -3/Drainage péricarde si Tamponnade -4/Sonde E.ESystolique si bradycardie -5/Drugs:Dobu, Dopa, diurétiques -6/ Assistance circulatoire ou Greffe coeur
TRAITEMENT • Choc hémorragique: -1/Rétablir la volémie -2/Assurer une oxygénation efficace -3/Transfusion sanguine si perte >25%: (Hb souhaitée -Hb observée)xP(kgs)x3,5 NB:250 ml de culot →↑1,2 Hb (adulte) Risque d’OAP, ↓Ca++,↑K+,Hémolyse,etc. -4/Correction des troubles de coagulation -5/ TTT de la cause de l’hémorragie
TRAITEMENT • Choc Anaphylactique: ADRENALINE+++ 1/ Corrige la vasoplégie 2/Corrige la bronchoconstriction. 3/Renforce l’inotropisme Rx VASCULAIRE ASSOCIE A L’ADRE 4/Reconnaitre l’allergène et liste au patient. 5/Port d’un KIT d’adrénaline auto-injectable
TRAITEMENT • Choc Septique: Grave/TTT Agressif-rapide 1/Rx Vasculaire <30ml/kg 2/Transfusion si Ht<30% ou 25% cardiaque 3/Prélévements infectieux 4/ANTB aveugle et adapté(antibiogramme) 5/Drugs: Levo, Dopa , Dobu 6/Corticoïdes précocément: HSHC
SURVEILLANCE CLINIQUE -1/Neuro: conscience -2/Cardiaque:FC, T.A,PVC -3/ respiratoire: FR, SpO2 (oxymètre) -4/Cutanés:marbrures -5/ T° -6/escarres, thromboseou lymphangite
SURVEILLANCE PARACLINIQUE • Gazo artérielle: RA, Pao2,Ph (Acidose) • Bilan rénal, hépatique, enzyme cardiaque • Radio du thorax:OAP, Sondes • ECG • Bactério
ETAT DE CHOC • Merci De Votre Aimable Attention