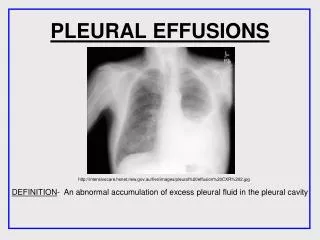
Pleural Effusions
Pleural Effusions. Sadie T. Velásquez , M.D. Case presentation.

Pleural Effusions
E N D
Presentation Transcript
Pleural Effusions Sadie T. Velásquez, M.D.
Case presentation 54-year-old man is referred because of progressive exertional dyspnea over a 1-month period. He has a 3-year history of type 2 diabetes mellitus that has been poorly controlled, with a hemoglobin A1c level of 7.4%. He was diagnosed with chronic pancreatitis 6 months prior to presentation. Medications include glycyron, glimepiride, and famotidine. He is a heavy alcohol drinker and has a smoking history of 34 pack-years. On Physical Examination his vital signs are normal except for dullness to percussion and decreased breath sounds over the left hemithorax. No cardiac murmurs are heard, and no clubbing and pitting edema are noted.
Laboratory examination shows a normal CBC count and transaminase levels, but mild elevations of amylase level (168 IU/L), lipase level (169 IU/L), glucose level (235 mg/dL), erythrocyte sedimentation rate (30 mm/h), and C-reactive protein level (2.9 mg/dL). The chest radiograph follows.
Enhanced thoracoabdominal CT scan reveals a massive left pleural effusion as well as a protruding, encapsulated, fluid-filled cystic lesion derived from the pancreatic tail.
The lesion is 24mm x 47mm in size and it expands upward, contacting the posterior gastric wall of the fornix along with the left crura of the diaphragm, connecting to the left thoracic cavity. Peripancreatic fat with a high-density area is also noted.
Thoracentesis fluid on the left side is black in color, and fluid analysis shows lactate dehydrogenase level 784 IU/L, total protein level 4.4 g/dL, glucose level 115 mg/dL, and hematocrit level 0.1%, consistent with an exudative pleural effusion. Cytology of the centrifugation sediment of the pleural fluid demonstrates RBCs in the background and a small number of neutrophils, and it is negative for malignancy. All cultures and stains for bacteria, including for mycobacteria and fungi, are negative. Further fluid study shows marked elevations of amylase level (5,292 IU/L), total bilirubin level (7.3 mg/dL; indirect bilirubin 6.5 mg/dL), and a pleural fluid-to-serum bilirubin ratio of 24:3, along with the presence of iron (223 m g/dL).
Diagnosis? Pancreaticopleural fistula with a pancreatic pseudocyst caused by chronic pancreatitis, causing a black pleural effusion generated by hemolysis of thoracic bleeding
BTS guidelines/CHEST Pleural effusions
Objectives • Discuss clinical assessment and history of a patient presenting with a pleural effusion • Discuss appropriate initial diagnostic imaging • Review algorithm for the investigation of unilateral and bilateral pleural effusions • Discuss indications for thoracentesis • Review diagnostic pleural fluid studies and how to differentiate between an exudative and transudative effusion • Review some specific conditions and tests • Management of pleural effusions after diagnosis
Clinical Assessment and History • Clinical assessment often capable of identifying transudates • ~75% of pulmonary emboli and pleural effusion have pleuritic pain • Drug history • Methotrexate • Amiodarone • Phenytoin • Nitrofurantoin • Beta-blockers • Occupational history • Asbestos exposure • Secondary exposures
Initial Diagnostic Imaging • Posteroanterior chest x-ray • Abnormal in the presence of ~200ml of pleural fluid • 50ml can produce detectable costophrenic angle blunting on a lateral film • AP supine exams result in free fluid lying posterior in the dependent portion • Subpulmonic effusions occur when fluid accumulated between the diaphragmatic surface of the lung and the diaphragm • May require ultrasound scan to diagnose • PA may show a lateral peaking of an apparently raised hemidiaphragm and lateral film may have a flat appearance of the posterior aspect of the hemidiaphragm
Bedside ultrasound guidance significantly increases the likelihood of successful pleural fluid aspiration and reduces the risk of organ puncture • Ultrasound detects pleural fluid septations with greater sensitivity than CT
N Engl J Med, Vol. 346, No. 25 · June 20, 2002 · www.nejm.org · 1973
Indications for Thoracentesis • Presence of clinically significant pleural effusion (>1cm thick on ultrasonography or lateral decubitus radiography with no known cause • Unilateral effusion • >3 days of pleural effusion despite diuresis in CHF
Tests Indicated, According to the Appearance of the Pleural Fluid
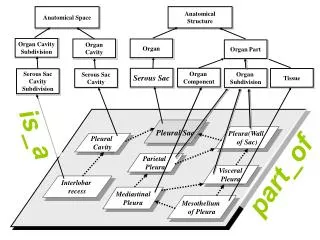
Diagnostic Studies • A TRANSUDATIVE pleural effusion occurs when pleural fluid accumulated because of an imbalance between the hydrostatic and oncotic pressures (increased plasma osmotic pressure or elevated systemic or pulmonary hydrostatic pressure) • An EXUDATIVE effusion occurs when the local factors influencing the accumulation of pleural fluid are altered (inflammation or other disease of the pleural surface)
http://www.merckmanuals.com/professional/pulmonary_disorders/mediastinal_and_pleural_disorders/pleural_effusion.htmlhttp://www.merckmanuals.com/professional/pulmonary_disorders/mediastinal_and_pleural_disorders/pleural_effusion.html
CHF and Pleural Effusions • Diuretic therapy increases the concentration of protein, LDH and lipids in pleural fluid and Light’s criteria are known to misclassify a significant proportion of effusions as exudates • Serum albumin – pleural fluid albumin >1.2g/dL • Protein gradient >3.1g/dL • Evidence for using BNP is scarce • NT-proBNP is effective in recognizing cardiac effusions that are misclassified by Light’s criteria (Porcel 2011)
N Engl J Med, Vol. 346, No. 25 · June 20, 2002 · www.nejm.org · 1973
Evaluation of Exudative Effusion • Total and Differential Cell Counts • Neutrophil predominant • Lymphocyte predominant • Eosinophilia • Pneumothorax • Hemothorax • Pulmonary infarction • Benign asbestos pleural effusion • Parasitic disease • Fungal infection • Drugs • Malignancy • Smear and Cultures • Pleural-Fluid Glucose Level • Glucose level <60mg/dL • Pleural-Fluid Lactate Dehydrogenase Level • Cytology • 65% yield on the first specimen and further 27% on the second and only 5% on the third • ≥ 60ml
Specific Conditions and Tests • Amylase • Acute pancreatitis • Chronic pancreatic pleural effusion • Esophageal rupture • Malignancy • Tumor markers: no single pleural fluid tumor marker is accurate enough for diagnostic evaluation • Markers of TB • ADA or interferon-gamma or PCR Salivary amylase
Hematocrit • Hemothorax: pleural fluid hematocrit >50% of the patient’s peripheral blood • Grossly bloody pleural fluid usually due to malignancy, PE with infarction, trauma, benign asbestos pleural effusions • NT-proBNP • pH • Pleural-fluid pH <7.2 with a parapneumonic effusion indicates the need for drainage • Pleural-fluid pH <7.2 suggests that the patient’s life expectancy is only about 30 days and pleurodesis is likely to be ineffective • Exposure of fluid to air increases the pH by ≥0.05 in 71% of samples and inclusion of 0.2ml of local anesthetic reduces the pH by 0.15
Cholesterol >250mg/dL • Triglycerides >110mg/dL supports the diagnosis of chylothorax and <50mg/dl excludes • Demonstration of chylomicrons confirms a chylothorax • Presence of cholesterol cyrstalsdianosespseudochylothorax
Further Diagnostic Imaging • Computed Tomography • With contrast • All undiagnosed exudative pleural effusions • All complicated pleural infection when tube drainage has been unsuccessful and surgery is to be considered • MRI • Distinguishes benign and malignant pleural effusions via differences in T2-weighted images
Management • Percutaneous pleural biopsy • Appropriate when investigating an undiagnosed effusion when malignancy is suspected and CT reveals pleural nodularity. Image-guided cutting needle is the method of choice. • Diagnostic rate of only 57% • Thoracoscopy • Investigation of choice in exudative effusions where a diagnostic pleural aspiration is inconclusive and malignancy is suspected. • Local anesthetic thoracoscopy (92% diagnostic sensitivity- can give talc for pleurodesis afterward) vs. • VATS (95% sensitivity- can do other thoracic surgical options at the time of procedure)
In all patients with acute bacterial pneumonia, the presence of a parapneumonic effusion should be considered • Patients with very low (category 1) or low (category 2) risk for poor outcome may not require drainage (level D) • Drainage is recommended for management of category 3 or 4 • Therapeutic thoracentesis or tube thoracostomy alone appear to be insufficient treatment for managing most patients with category 3 or 4 PPE • Fibrinolytics, VATS and surgery are acceptable approaches for managing patients with category 3 and 4 PPE
Malignant Effusions • Median survival 3-12 months • Majority are symptomatic (75%) • Massive pleural effusions most often caused by malignancy • Options for management: • Observation • Therapeutic pleural aspiration (not recommended if life expectancy >1 month) • Intercostal tube drainage and instillation of sclerosant • Thoracoscopy and pleurodesis • Placement of an indwelling pleural catheter
VA Wards Cases from this month…
Appearance: clear yellow • Serum LDH 188, total protein 5.7, albumin 2.3 • Pleural Fluid Cell Count: WBC 38% segs, clotted • Pleural Fluid: pH 7.5, LDH 45, cholesterol 14, amylase 16, triglycerides <10, albumin <1.2, t prot <3, glucose 206
Diagnosis? • LDH fluid/LDH serum= 0.23 • Tprotein fluid/Tprotein serum= 0.53 (but protein in fluid <3) • Serum albumin-pleural-fluid albumin= 1.1 (but albumin in fluid <1.2) • Serum albumin – pleural fluid albumin >1.2g/dL