Download
1 / 23
240 likes | 511 Views
Management of Pleural effusions HUEH 2011 Terry Flotte, MD. Case Presentation. 4 year-old female presents with 5 days of fever, worsening tachypnea, some abdominal pain. Temp 40.2C, RR 48, pulse oximetry 89% Absent breath sounds and dullness right lung base

E N D
Case Presentation • 4 year-old female presents with 5 days of fever, worsening tachypnea, some abdominal pain. • Temp 40.2C, RR 48, pulse oximetry 89% • Absent breath sounds and dullness right lung base • Decrease in whispered pectorloquy, vocal fremitus
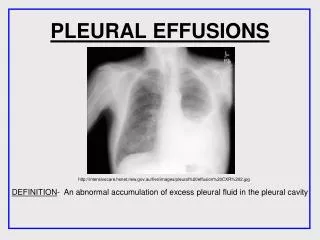
Etiology of pleural effusions: exudative • Exudative (*High protein, High LDH) • Para-pneumonic: Bacterial • Early Exudative • Fibrinopurulent • Empyema (pus, pH<7.2) • Tuberculous • Non-infectious • Pancreatitis • Lupus *Protein > 0.5 serum protein; LDH > 250; LDH >0.6 serum LDH (can use SG >1.015)
Other causes • Transudative (low protein/ low LDH) • Congestive heart failure • Nephrotic syndrome • Other • Chylous (high triglycerides) • Congenital • Thoracic duct injury • Iatrogenic • Hemothorax (blood) • Trauma • Malignant
Bacterial Pneumoniascausing Parapneumonic effusions • Pneumococcus (S. pneumoniae) • Staphylococcus aureus (including MRSA) • S. pyogenes (Group A beta-strep) • Anaerobic Infections • H. influenzae • Other: Klebsiella, Pseudomonas, Legionella • TB and atypical mycobacteria
Value of decubitus films Upright Right side down Layering Left side down Clearing of Right base
Parapneumonic effusions • Good prognosis without tube drainage • Appearance (thin yellow) • Labs (high pH, lower LDH, higher glucose) • Non-loculated • Worse prognosis without tube drainage “empyema” • Thick Pus • Loculated
When and How to do thoracentesis • Large effusions • Effusions with excessive dyspnea or hypoxemia • Diagnostic questions
Tuberculous Effusions • Thought to arise from rupture of subpleural caseous focus • Frequent in early, untreated cases, with concomitant HIV • Meets criteria of Exudative Effusion but with a greater proportion of lymphocytes in fluid • Pleural fluid smears and cultures are often negative
A few notes about chylothorax • Most common cause of neonatal effusion • Birth trauma to Thoracic duct • Congenital • Post-surgical or other trauma • Associated with lymphangiomatosis • Iatrogenic with central venous infusion of lipid
Management of Chylothorax Maintaining Nutrition and Reducing the Volume of Chyle Circulation Dietary: medium-chain triglyceride diet or total parenteral nutrition OctreotideRelieving Dyspnea by Removing Chyle from the Pleural Cavity Thoracentesis (short term only) Tube thoracostomy (short term only) Pleuroperitoneal or pleurovenous shunting PleurodesisTreatment of the Underlying Defect Thoracic duct embolization Ligation of the thoracic duct (thoracoscopy or thoracotomy) Clipping or fibrin glue to the thoracic duct leak Radiotherapy for mediastinal lymphoma
Sources • Murray and Nadel’s Textbook of Pulmonary Diseases • Diseases of the Pleura • Nelson’s Pediatrics