Download
1 / 47
540 likes | 671 Views
Learn about pleural anatomy, pleural effusions, and the mechanisms, symptoms, and diagnosis of pleural disease. Explore thoracenthesis, radiology, and biochemical evaluations for effective treatment.

E N D
PLEURAL DISEASE Sevda Özdoğan MD, ChestDiseases
Pleural effusions • Emphyema • Pleural malignancy • Hemothorax • Pneumothorax
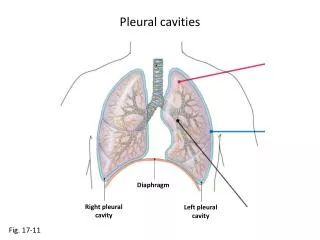
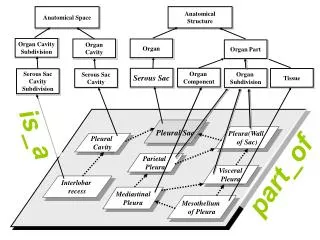
Pleural Anatomy and Physiology • Pleura is a serous membrane formed from mesenchyme that separates the lung paranchym, mediastinum, diaphragm and thoracic cage • It is composed of 2 layers as: • Parietal pleura • Visceral pleura
Pleural Cavity • It is the space between the visseral and parietal pleura • Normally contains a small amount of fluid (10-20 ml in each pleural cavity) • This pleural fluid is mainly produced by the parietal pleural surface and reabsorbed by the two layers (Mainly parietal pleura)
The production and reabsorbtion of the pleural fluid is normaly in an equilibrium accounted primarily by the forces employed in Starling equation: F=k[(Pcap-Ppl)-δ(πcap- πpl)] F: The rate of fluid movement P, π: Hydrostatic and oncotic pressures k: The filtration coefficient δ: Osmotic reflection coefficient
PleuralEffusion • Ifthephysiologicbalancebetweenthefiltrationandthedrainage of thepleuralfluid is disturbed, pleuraleffusionaccumulate. • Fluidmayaccumulate in thepleuralspace in responsetothedisease of thepleuralmembranesor as a manifestation of a systemicillness
The Mechanisms of Pleural Effusion • Increased hydrostatic pressure (Cardiac failure, increased atrial pressure) • Decreased oncotic pressure (Protein deficiency) • Decreased pleural cavity negative pressure (Atelectasis) • Increased permeability in microvascular circulation (İnfections, inflammation) • Impaired lymphatic drainage of pleural space (Tumor, fibrosis) • Transperitoneal route (Congenital defects, ascite)
Symptoms • Chest pain (inspiratory) • Decreases when the fluid increases • Dyspnea • Cough • Symptoms of the underlying disease • Fever • Hemoptysis • Weight loss • ...
Physical Examination • No physical signs can be detected when the fluid is less than 300 ml • İnspection • İncreased size of the affected hemithorax • Trachea is deviated away from the diseased side
Palpation • İpsilateral restriction of chest wall motion • VT absent • Percussion • Dullness (>300-400 ml) • Oscultation • Diminished breath sounds or inaudible • Pleural friction rub • Bronchial sound over the fluid level
Radiology • The fluid initially accumulates in the more dependent recesses of the thoracic cavity forming a Damoiseau Line • 200-300 ml of pleural effusion can be detected on standard chest radiograph as blunting of the costophrenic angle
MassivepleuralfluidoftenshiftsthemediastinumtotheoppositesideMassivepleuralfluidoftenshiftsthemediastinumtotheoppositeside • Unusuallocalizedpleuraleffusions can be seenduetothelocalizedobliteration of thepleuralspaceoften by inflammatoryconditions (adherence)
Smaller amounts of pleural fluid can be detected on lateral decubitus radiography as the free intrapleural fluid moves from top of the diaphragm to the dependent chest wall Pleural effusion in a lateral decubitus radiograph
Ultrasound is able to demonstrate smaller amounts of fluid as 100 ml • CT has similar sensitivity to ultrasound, not routine but can be performed to evaluate concomitant paranchymal lesions • CT is sensitive in identifying pleural thickening and calcification
Thoracenthesis and Pleural Fluid analysis • Appereance • Serous (lighttodarkyellow, clear) • Serosangineous (Blood tinged can be duetothoracentesisitself) • Hemorrhagic (hemothoraxifhct>50% of bloodhct) • Purulent (fetidodor in unaerobicinfections) • Chylous (milky)
Biochemicalevaluation • Exudative • Transudative • Somespecialhints • Microbiologicalevaluation • Cellular structure • Special stainsandculture • Cytologicevaluation
Routine pH Glucose Lactate dehydrogenase Total protein Albumine Optional Htc Cholesterol Trigliserid Bilirubine Adenosin deaminase Amylase RF LE cell ANA Hyaluronic ascite Biochemical Evaluation
Exudate Dark yellow color Total protein >3 gr/dl Density >1016 Light Criteria: Protein pl/s >0.5 LDH pl/s >0.6 LDH >200 or >2/3 of normal upper value of serum Transudate Light yellow color Total protein <3 gr/dl Density <1016 Light Criteria: Protein pl/s <0.5 LDH pl/s <0.6 LDH <200 Biochemical Evaluation
Albumine Gradient: • Serum albumine- Pleural fluid albumine • <1.2 gr/dl Eksudate • >1.2 gr/dl Transudate • Pleural Cholesterol >60 mg/dl: Eksudate • Pl/S bilirubine >0.6: Exudate
Transudative Pl. Eff. Increased hydrostatic pressure Congestive heart failure Constrictive pericarditis Pericardial effusion Pulmonary thromboemboli Decreased oncotic pressure Cirrhosis Nephyrotic syndrome Malnutrition Increased capillary permeability Myxedema Pulmonary thromboemboli Transperitoneal transport Peritoneal dialysis Ascites Exudative Pl. Eff. Infectious diseases Pnomonia, lung abscess Tuberculosis Fungal infections Subphrenic abscess Neoplastic diseases Metastatic Mesothelioma Lymphoma Immunologic reactions Dressler syndrome Sistemic Lupus Er. Rheumatoid artritis Churg strauss syndrome Wegener granulomatosis
Exudative Pl Eff Gastrointestinal disease Pancreatitis Causes of peritoneal exuda Drug induced Nitrofurantoin Dantrolene Methysergide Bromocriptine Procarbasine Amiodorone Postsurgical Pulmonary thromboembolism
ExudativePlEff Sarcoidosis Uremicpleuritis Asbestosexposure Chylothorax Hemothorax
Iftheeffusion is transudativethe main causeshould be treated • Iftheeffusion is exudativeand not emphyemafurtherdiagnosticproceduresshould be considered • Cytologicexamination • Closedpleuralneedlebiopsy • Thoracoscopy (VATS) • Thoracotomy
Chylothorax Triglyceride >110 mg/dl Pl TG/sTG>1 Cholesterol crystal (-) Pl Ch/s Ch<1 Chylomicrons (+) Pseudochylothorax Triglyseride <50 mg/dl Pl TG/sTG<1 Cholesterol>250 mg/dl Pl Ch/s Ch>1 Emphyema PH<7.20 Low Glucose Special characteristics:Milky appearance
Microbiologic evaluation • RBC >100 000/mm3 • Trauma, • Pulmonary infarction • malignancy • WBC > 1000/mm3 : exudate > 10 000/mm3 : emphyema, parapnomonic effusion (PNL predominates) Mesothelial cells<5%: tuberculosis possible Lymphocytes >50% : tuberculosis, malignancy, lymphoma, fungus, myxedema
Gram staining • Ziehl-Neelsen staining • Cultures for specific and nonspecific infections • PCR
Infectious pleuresy, emphyema • Bacterial pneumonia is associated with an effusion in 40% of cases • The effusion may be parapneumonic without infection (uncomplicated) or culture positive (complicated, emphyema) • Parapneumonic effusions are treated with appropiate antibiotics • Tube drainage is indicated if emphyema occurs
Other Pleural Diseases • Hemothorax • Plevral fluid htc>50% of serum • Can be traumatic or nontraumatic: • İatrogenic • Pulmonary infarction • Tumors • Rupture of aneurism • Anticoagulan treatment • Thoracic endometriosis • Treatment: • intrapleural drainage • thoracotomy
Fibrothorax • A thick fibrous tissue formed on visceral pleura • Cause: • Empyema • Tuberculosis • Hemothorax • Treatment: Decortication
Pneumothorax • Presence of free air between the visceral and parietal pleura • Divided into 3 • Spontaneous • Primary idiopathic • Secondary • Traumatic • Iatrogenic
Primary Spontaneous Pneumothorax • Mostly occurs in young, male, smokers • There is no obvious underlying pulmonary disease • Subpleural blebs and bullae probably play a role in pathogenesis • Symptoms can be an acute unset of dyspnea and unilateral chest pain but can be absent also depending on the size of the pneumothorax
Physical examination: • Hypersonority on percusion • Reduced breath sounds, reduced VT, enlarged hemithorax • Hypotension and cardiac tamponade may occur depending on the size of the pneumothorax • Radiology: • Pleural line • Hyperlucency at the periphery • Mediastinal shift • Expiration film can be used when the lesion is not apparent
Quantification of the size of the pneumothorax is helpfull in the decision of treatment • Measurement of the average diameters of the collapsed lung and the affected hemithorax can be used • 100-(83/113)100=% 62 • Simple observation with rest and supplemental oxygen can be used for asymptomatic patients with a small (<20%) px • Intercostal drainage is indicated in large px • A recurrent spontaneous pneumothorax (30-50% risk) is an indication for surgery
Secondary Spontaneous Pneumothorax • Patientshave an underlyingpulmonarydisease: • COPD • Asthma • Congenitalcystsandbullae • Interstitiallungfibrosingdiseases • Cysticfibrosis • Hystiocytosis X • Whoopingcough • Lymphangiomyomatosis • Pleuralendometriosis, catamenialpneumothorax • Pleuralmalignancy • Sarcoidosis • BacterialpneumoniaandPneumocystisPneumonia
Traumatic and Iatrogenic Pneumothorax • Iatrogenic pneumothorax can be seen during: • Thorasentesis • Pleural needle biopsy • Transthoracic lung aspiration biopsy • Mechanical ventilation • Central venous catheterization • Tracheostomy • Cardiopulmonary resusitation
Pleural Neoplasms • Benign: • Pleural lipoma • Local pleural fibroma (Fibrous mesothelioma) • Malign: • Diffuse malign mesothelioma
Malign Pleural effusions • Diffuse Malign Mesothelioma • Bronchial carcinoma (adenocarcinoma) • Lymphoma • Breast carcinoma • Other adenocarcinomas
Malignant Mesothelioma • Primary tumour of pleural, pericardial, peritonial mesothelium • Etiology: 70-90% asbest exposure: • Occupational: asbest is resistant to heat and friction so used in building, water pipes, brakes, isolation systems, textile • Environmental: Eskişehir, Kütahya, Bilecik, Yozgat, Sivas, Diyarbakır • Latent period is 30-40 years in occupational exposure • Smoking dramaticaly increase the risk of cancer in asbest exposure
Erionite is another fibrous zeolite found in soil, high in Nevşehir: Tuzköy, Karain, Sarıhıdır area in Turkey. It is more carcinogenic than asbest. 49% of total deaths in the villages of Ürgüp are due to DMM
The most common clinical presentations are dyspnea, chest pain, unilateral decreased volume of the affected hemithorax (frozen chest) (inspite of fluid accumilation) • Nodular thickening of the pleura, irregular thickening of the interlobar fissure, absence of mediastinal shift with massive pleural effusion (frozen chest) • Diagnosis by histologic examination • Treatment oncologic and surgical if possible, prognosis is poor