Download
1 / 16
330 likes | 2.81k Views
. Q.1- the clinically important important diameter in pelvic inlet is: 1-true conjugate 2-obesteric conjugate 3-diagunal conjugate 4- all of the aboveQ.2- most common type of pelvis is 1- gynecoid 2-anthropoid 3-platlypelloid 4-androidQ.3-the narrowest diameter in the pelvis is 1-interspinous 2-anteroposterior of mid pelvis 3-obliq197

E N D
1. Anatomy of the bony pelvis Lateefa Al Dakhyel FRCSC, FACOG
Assistant professor & consultant
Obstetric & gynecology department
Collage of medicine
King Saud University
2. Q.1- the clinically important important diameter in pelvic inlet is:
1-true conjugate
2-obesteric conjugate
3-diagunal conjugate
4- all of the above
Q.2- most common type of pelvis is
1- gynecoid
2-anthropoid
3-platlypelloid
4-android
Q.3-the narrowest diameter in the pelvis is
1-interspinous
2-anteroposterior of mid pelvis
3-oblique diameter
4.obestric conjugate
Q.4-Which statement is incorrect
1-adequcy of female pelvis for labor can be accurately assessed by CT scan
2. progress of labor is the true assessment of female pelvis
3.labor dystocia can caused by android pelvis
4.intra labor pelvic assessment can be done
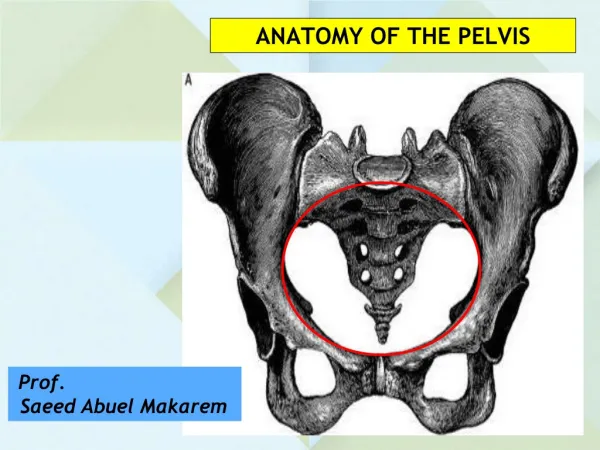
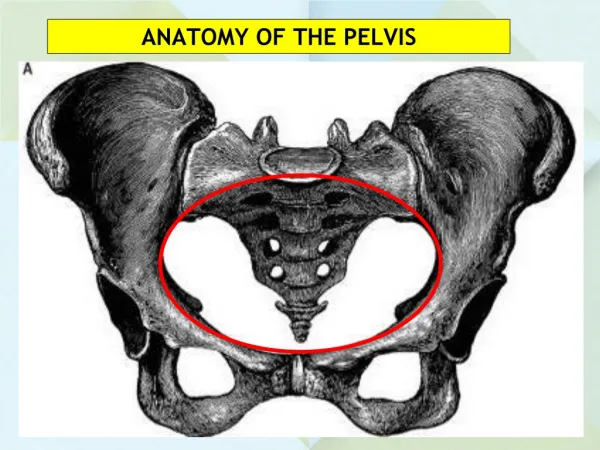
3. Female bony pelvis False pelvis
lies above the linea terminalis (pelvic brim)
has no obstetrical significance.
True pelvis
Lies below linea terminalis (pelvic brim)
has important role in child birth
It has inlet, cavity & outlet
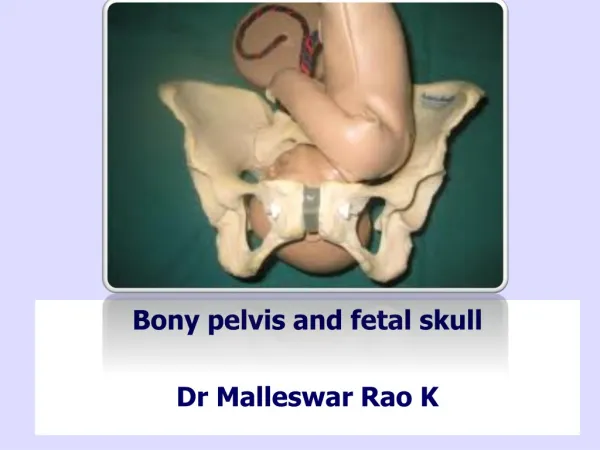
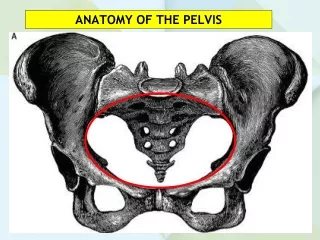
4. True pelvis Pelvic inlet (superior strait)
boundaries: a. rami of Pubic bone, symphysis pubis
p. sacral promontory
l. linea terminalis
diameters:
1.anteroposterior diameter
obstetrical conjugate:
shortest distance between the promontory and symphysis pubis
normally measures 10cm or more.
(others: true conjugate & diagonal conjugate)
2.The transverse diameter
greatest distance between linea terminalis on either side
3.Rt & Lt oblique diameter
extend from one of the sacroiliac synchondroses to the iliopectineal eminence on the other side
6. Mid pelvis
-at the level of ischial spines
-interspinous diameter usually ~10cm
- Smallest diameter of the pelvis
7. Pelvic outlet
-boundaries a. the area under the pubic arch
p. the tip of the sacrum
l. ischial tuberosities, sacrosciatic ligments
-diameters
1.Anteroposterior diameter(9.5-11.5)
from the lower margins of the symphesis pubis to the tip of the sacrum
2. The transverse diameter (11cm)
the distance between the inner edges of the ischial tuberositis.
3.The posterior sagittal diameter (>7.5)
from the tip of the sacrum to the line between ischial tuberositis
9. Pelvic shapes Caldwell-Moloy classification
-A line drawn through the greatest diameter of the inlet divides it to ant. & post.
10. Gynaecoid pelvis:
It is the commonest type (50%)
Inlet is slightly oval or round (TD~APD)
Sacrum is wide with average concavity and inclination.
ischial spines not prominent (transverse diameter is = >10cm)
Sacro-sciatic notch is wide.
wide pubic arch
11. Anthropoid pelvis:
It makes 25% of white & ~ 50% of nonwhite women.
All anteroposterior diameters are more than transverse diameters (Oval anteroposteriorly)
Ischial spines mostly prominent.
Sacrum is long and narrow.
Sacro-sciatic notch is wide.
Subpubic angle is narrow.
12. Android pelvis :
It is~ 30% of white & ~15% 0f nonwhite women.
Inlet is triangular or heart-shaped with anterior narrow apex.
Side walls are converging (funnel pelvis) with projecting ischial spines.
Sacro-sciatic notch is narrow.
Subpubic angle is narrow <90o.
The extreme android pelvis have poor prognosis for vaginal delivery.
13. Platypelloid pelvis :
It is a flat female type, it is rarest ~3% of women only.
All anteroposterior diameters are short.
All transverse diameters are long (oval transverse)
Sacro-sciatic notch is narrow.
Subpubic angle is wide.
The sacrum usually is well curved and rotated backward.
14. Intermediate-type pelvis
mixed types are much more frequent than pure types.
significant clinical points
-obstructed labor caused narrowing of midpelvis or pelvic outlet
-obstetric conjugate can be measured radiological only, diagonal conjugate can be estimated clinically
-ischial spins can be felt with vaginal exam
-most important test for pelvic adequacy is labor progress it self
15. Clinical estimation of pelvic size
16. Best test of pelvic adequacy is progress of labor it self
History of vaginal delivery of average weight fetus means the pelvic is
adequate.
Pelvic inadequacy: -big baby
-small pelvis
-abnormal position