Thyroid gland
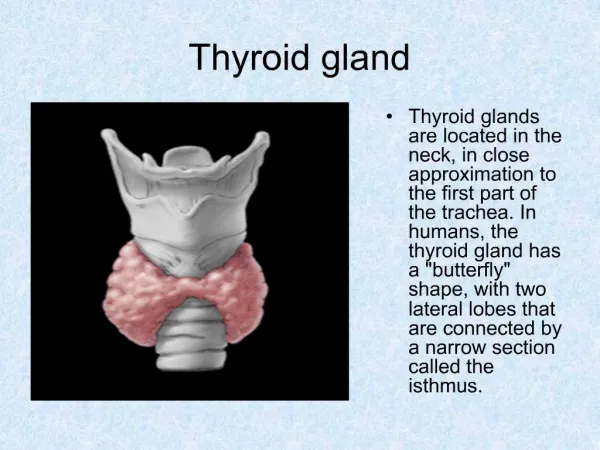
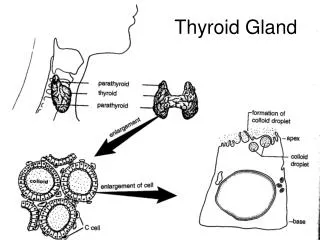
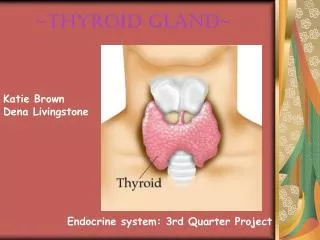
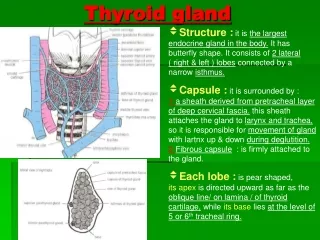
Thyroid gland. Anatomy. Bi-lobed gland over second and third tracheal ring piramidal lobe : 40 – 50 % Weight : 20 – 30 gr Epithelium lined follicle Colloid : glycoprotein ( thyroglobulin ) Vascular stroma True connective tissue capsule .

Thyroid gland
E N D
Presentation Transcript
Bi-lobed gland over second and third tracheal ring • piramidal lobe : 40 – 50 % • Weight : 20 – 30 gr • Epithelium lined follicle • Colloid : glycoprotein ( thyroglobulin ) • Vascular stroma • True connective tissue capsule
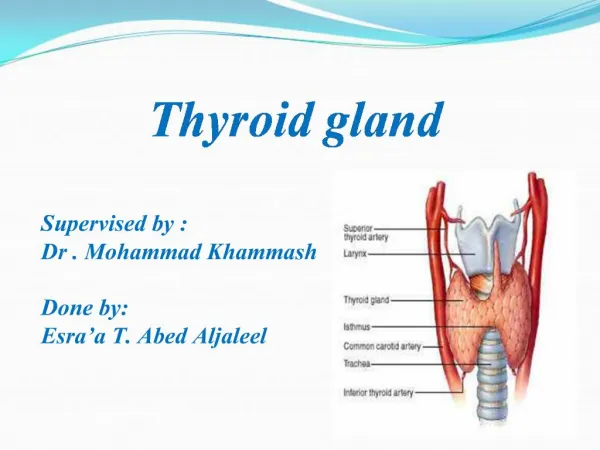
It is important to ligate the superior thyroid artery close to the gland to avoid injury to the nerve during thyroidectomy
Inferior thyroid artery • Inferior thyroid artery : Thyrocervical trunk Absent in up to 6% • Thyroidea ima : directly from aorta , innominate artery or right common carotid artery • Present in up to 12%
Superior thyroid vein : IJV or common facial vein • Inferior jugular vein : innominate vein or IJV • Middle thyroid vein : IJV • Lymphatic → paratracheal nodes → superior mediastinum & middle deep cervical node and lateral the neck
Embryology • Median endodermal derivative that migrates from the tongue base to its normal position in the neck by 7th week . • The distal portion of this thyroglossal duct forms the thyroid gland
Physiology • Concentrate iodine • 20 – 30 % is store in thyroid • Small percentage in hormone and nonthyroid tissue • All tyrosine compounds are bound to thyroglubulin and store in thyroid follicles as colloid • The unbound thyroid hormone is responsible for influencing metabolism .
Thyroglossal duct anomaly • 7% of the population has remnants of the thyroglossal duct • Cyst : anywhere along the length of duct 60% infrahyoid , 24% suprahyoid , 1% intralingual • 1-2 cm cystic mass that is mobile on swallowing & protruding of the tongue
60% contain thyroid tissue • Malignancy is rare • Acute infection • Contain mucus like clear fluid • If it is become symptomatic it must be removed • Sistrunk operation
Lingual thyroid • Failure of thyroglossal duct to descend • A mass at the foramen cecum • Aysmptomatic or present with airway obstruction • May be the only thyroid tissue
Ectopic thyroid tissue • Anywhere along the migratory route of the thyroid • Mediastinum , larynx , trachea , pericardium or esophagus
Congenital intrathyroid cysts Present in children persistent ultimobranchial bodies or an intrathyroidal thyroglossal duct cyst
Acute suppurative thyroiditis • M=F • Preceded by an upper respiratory tract infection • Staph. The most common organism • Painful enlargement of the gland • Fever • Abscess formation
Sporadic form • More common in female • Difuse thyroid enlarement • Without pain or thyroid enlargement • Temporary hyperthyroidism • 50% become hypothyroid which resolves in 6 month
Postpartum thyroiditis • Initial hypothyroidism is mild • Lymphocytic infiltration and follicle disruption • Self-limiting disease • Steroid may be of value
Subacute thyroiditis ( De Quervain´thyroiditis ) • At all age most common at 5th decade • F>M • May be viral • Painful thyroiditis • Defuse thyroid enlargement • Malaise and fever • thyrotoxic
Endocrine phases • Hyperthyroidism : 1-3 month • Euthyroid : 1-3 weeks • Hypothyroid : 2-6 month • Recovery which is complete
Lymphocyte , monoycyte and giant cell infiltration . • Treatment consist of analgesic steroid and antiinflammatory agents .
Hashimoto´s thyroiditis • Common • Affecting 2 population • 95 % in female Autoimmune etiology with strong genetic predisposition • Diffusely enlarge with nodularity firm • Disrupted follicle with lymphocyte and plasma cell infiltration and variable fibrosis • Residual hypothyroidism
Anti thyroglobulin and antimicrosomsal ab are present up to 90% • FNA is diagnostic • Increased risk for developing B – cell lymphoma
Riedel‘s thyroiditis • Uncommon • F>M • Older patient • May be mediastinal & retroperitoneal fibrosis • Fixed rock-hard thyroid enlargement • Gland replaced with fibrosisAirway obstruction and dysphagia • Palliative surgery to relieve obstruction
Graves‘ Disease • 3th and 4th decade • F/M : 7/1 • Autoimmune etiology : abnormal Ig that fix on TSH receptor of thyroid epithelial cell • Diffuse toxic goiter • ophthalmopathy 55% • Dermophathy 5%
Cont. • ↑ T3 , T4 , T3RU • Thionamide , sympathetic blocker , iodine • Radioactive iodine
Surgical indication • Refuse radioactive therapy • Thyroid nodules suspicious for malignancy • Must be rendered euthyroid prior to surgery
Subtotal thyroidectomy leaving 7-8 gr of nodule free tissue is recommended however , total thyroidectomy is proposed by many
Toxic multinodular goiter • Older patient no ophthalmopathy or dermophathy • Total thyroidectomy • Radioactive iodine but not successfully as surgery
Toxic adenoma • Younger patient Quite large ( 2.5 – 3 cm ) • Surgical excision
Multinodular nontoxic goiter • Compensatory response • Common in female Secondary to dietry deficiency • Symptom and sign of pressure
Treatment • Thyroid suppression • Surgery: cosmetic deformity pressure symptom refractory to suppression Fear of malignancy Development of toxicity
Benign adenoma • Encapsulated tumor • Glandular epithelium with intratumoral degenerative changes ( hemorrhage , fibrosis , calcification ) • Rare thyrotoxicosis • Type : follicular,colloid , embryonal, fetal , Hurthle ???
Papillary carcinoma60 – 65 % • Third – 5th decade • F/M : 2/1 • Indolent with overall excellent prognosis • May arise from benign adenoma • Low-dose and high dose external RT
Macroscopic pattern • Occult ; <1.5 cm • Intrathyroid ( 70% ) • Extrathyroid : infiltrate larynx , trachea , strap muscle , great vessel
Microscopic pattern • Purely papillary • Some may have area of follicular • Anaplastic transformation is rar • Venous invasion in 10%
Intraglandular lymphatic invasion results in high incidence of multicentricity
Neither multicentricity nor regional LN metastasis have any prognostic significance
Negative prognostic indicator • Advance age • Male gender • extrathyroid extension • Distant metastasis
Cont. • Dedifferentiation • Vascular invasion • Atypical variants ( tall cell, columnar , sclerosing ) may have negative prognostic significance
Follicular carcinoma15% • Vascular invasion • Metastasis to bone brain and liver • Anaplastic transformation is more common • Overtly invasive : infiltrate surrounding structure ( MR 20-50%) • Minimally invasive : microscopically has capsular invasion (MR 5%)
Definitive diagnosis can often be established only on permanent section
Poor prognostic indicator • Advanced age • Male gender extrathyroid extension • Distant metastasis • Vascular invasion • anaplastic transformation trabecular growth pattern
Hurthle cell carcinoma 5% • As a variant of follicular tumors • Overtly invasive :higher mortality rate Higher LN metastasis • Minimally invasive