Download
1 / 8
80 likes | 262 Views
Eastern Europe & Central Asia 1.4 million [920 000 – 2.1 million]. Western & Central Europe 610 000 [480 000 – 760 000]. North America 1.0 million [540 000 – 1.6 million]. East Asia 1.1 million [560 000 – 1.8 million]. North Africa & Middle East 540 000 [230 000 – 1.5 million].

E N D
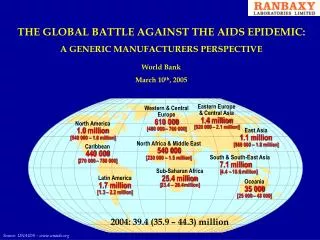
Eastern Europe & Central Asia 1.4 million [920 000 – 2.1 million] Western & Central Europe 610 000 [480 000 – 760 000] North America 1.0 million [540 000 – 1.6 million] East Asia 1.1 million [560 000 – 1.8 million] North Africa & Middle East 540 000 [230 000 – 1.5 million] Caribbean 440 000 [270 000 – 780 000] South & South-East Asia 7.1 million [4.4 – 10.6 million] Sub-Saharan Africa 25.4 million [23.4 – 28.4 million] Latin America 1.7 million [1.3 – 2.2 million] Oceania 35 000 [25 000 – 48 000] 2004: 39.4 (35.9 – 44.3) million THE GLOBAL BATTLE AGAINST THE AIDS EPIDEMIC: A GENERIC MANUFACTURERS PERSPECTIVE World Bank March 10th, 2005 Source: UNAIDS – www.unaids.org
Regional HIV/AIDS statistics: 2004 Scope of the global challenge • Fact: • UNAIDS estimate: 39.4mn PWA; year end 2004 • 6% Children ; 45% Women • 4.9mn newly affected in 2004 • 3.1mn deaths in 2004 14,000 new HIV infections per day Global estimates for adults and children: 2004 Worldbank; March 10th, 2005
Elements of the solution Worldbank; March 10th, 2005
Supporting Organizations Worldbank; March 10th, 2005
“The hurdles” • Formulate ARVs that are bio-equivalent to existing brands that can be manufactured in a more cost-effective manner. • Generate scientific data to support bio-equivalency for review by US FDA (as per PEPFAR guidelines). • Gain FDA approval and establish channels for distribution through supply chain consortiums. • Manufacture product to meet the requirements of healthcare systems to support patient care. • Address equivalency and quality questions. Worldbank; March 10th, 2005
The Ranbaxy Plan • Majority of 16 ARV dossiers to be submitted to the US FDA by Summer ‘05. • Cooperative scientific effort required between Active Pharmaceutical Ingredient (API) supplier; Ranbaxy formulation scientist and manufacturing groups. • Work with independent CRO to generate required data. • Data submitted to WHO concurrently for inclusion in drug listing. Worldbank; March 10th, 2005
The Ranbaxy Comittment • “We are well aware and applaud the fact that your administration, in the interest of protecting patients, has implemented an FDA review process for all generic ARV drugs used in the PEPFAR initiative, an important measure for patient safety…………. We plan to complete our bio-equivalence studies for our entire portfolio of ARVs within the coming year. Our current plans are to manufacture all PEPFAR-approved ARVs at Ranbaxy Laboratories Ltds’ FDA inspected and certified facilities to ensure the highest quality manufacturing environment” • Letter to Secretary Tommy G. Thompson • US Department of Health and Human Services • Brian W. Tempest. PhD. • Managing Director and CEO • Ranbaxy Laboratories Ltd. • January 2005 Worldbank; March 10th, 2005