Download
1 / 26
270 likes | 518 Views
Julie Wegner, PhD, CP Midwestern University Glendale, AZ. Hemostasis, platelets and Blood management. Disclosure. None. Why do patients bleed?. Macrovascular Microvascular Inability to generate thrombin Insufficient clotting surface (platelets)

E N D
Julie Wegner, PhD, CP Midwestern University Glendale, AZ Hemostasis, platelets and Blood management
Disclosure None
Why do patients bleed? • Macrovascular • Microvascular • Inability to generate thrombin • Insufficient clotting surface (platelets) • Insufficient substrates (clotting factors) • Inhibitors (anticoagulants, antithrombotic agents) • Clot not strong enough • Insufficient thrombin generation • Weak fibrin-platelet mesh (platelets, fibrinogen) • Clot vulnerable to lysis
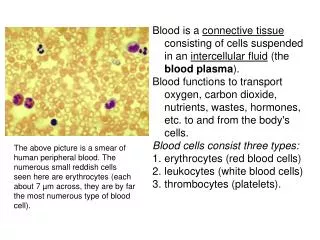
Hemostatic components Clot formation requirements Generating environment Provide substrate Provide protection Substrates for: thrombin generation fibrin formation Procoagulant factors Intrinsic Extrinsic Anticoagulant factors Antithrombotic factors Platelets Endothelium WBC RBC Endothelium Subendothelium Clot location
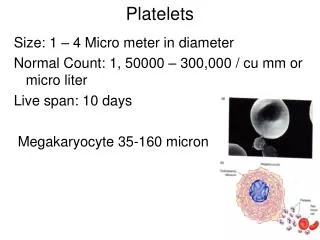
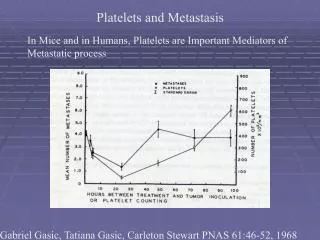
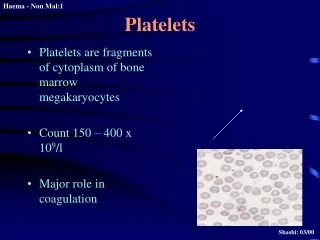
Platelet contributionInitiation and propagation Serial samples Cancer patients Correlations: platelet count vs. MA r=0.7 vs. R r=-0.7 vs. r=0.8 Roeloffzen WWH et al. Thrombocytopenia affects plasmatic coagulation as measured by thromboelastography. Blood Coag Fibrinolysis 2010 (in press).
Platelet cascade Adhesion http://www.integrilin.com/popups/platelet2.html
Insufficient clotting surface Insufficient substrates Presence of inhibitors Thrombin generation andhemostasis
Central role of thrombin From: Crawley JTB et al. The central role of thrombin. J Thromb Haemost. 2007; 5(Suppl 1): 95-101.
Thrombin generationkinetics T1 = lag phase T2 = maximum rate of TG T3 = Peak [thrombin] T4 = Total free thrombin (AUC) Fibrin cross linking Lateral aggregation TG = thrombin generation, AUC = area under the curve = endogenous thrombin potential (ETP) from: Wolberg AS. Blood Rev. 2007.
Thrombin generating surfaceThrombin generation and platelet # From: Vanschoonbeek K, Feijge MAH, van Kampen RJW et al. Initiating and potentiating role of platelets in tissue factor-induced thrombin generation in the presence of plasma: subject-dependent variation in thrombogram characteristics. J Thromb Haemost. 2004; 2:478-484.
TG and [substrate] Bollinger D et al. Br J Anaesthesiol 2009; 102:793 PPP (50%) No change in lag time Slight decrease rate TG Decrease peak TG
Decrease coagulation factors • FV and FVII ~ 28% Dilution • FII and FX ~ 44% Dilution + consumption • Thrombin potential – [FX] and [FII]-dependent • Blood loss vs. thrombin potential (r = -0.75*)
Post-op bleeding:Hemodilution vs. consumption? • Hemodilution global (cells and factors) • Consumption → global? • Importance of adequate anticoagulation • ACT @ 480 sec: clots vs consumption?
Heparin and thrombin generation Peak thrombin Max. rate thrombin generation Lag time From: Tanaka KA, Katori N, Szlam F, Sato N, Kelly AB, Levy JH. Effects of tirofiban on haemostatic activation in vitro. Br J Anaesth. 2004; 93:263-269.
Reversing heparin effectIs more protamine always good? • Fine tuning protamine • ‘excess’ protamine: TG • ‘excess’ protamine: • Increased time to clot • Decreased clot strength • Enhanced vulnerability to fibrinolysis Ni Ainle F et al. Blood 2009; 114:1658 Celite TF Nielsen VG. Ann Thorac Surg 2006; 81:1720
Insufficient thrombin generation Insufficient substrate (fibrinogen) Weak fibrin-platelet mesh (platelets) Weak clots
Thin Thick Fiber thickness Fiber weave Loose Tight Clot quality and [thrombin] Low Clot strength High Wolberg, AS. Thrombin generation and fibrin clot structure. Blood Review 2007; 21: 131- 142
Anesth Analg. 2010 In press 1 g/L 100 Plateau effect 120 x 109/L Bleeding • Depends on clot strength (MA) • fibrinogen levels • platelet function
Clot strengthFibrinogen vs. platelets Velik-Salchner C et al. JTH 2007; 5:1019 Lang T et al. Anesth Analg 2009; 108:751
Importance of clot strength in hemostasis Clot vulnerability to lysis
Fibrinolysis contact activation endothelium X I TAFI Thrombin http://www.setma.com/article.cfm?ID=330 Holly, J. Cardiometabolic Risk Syndrome Part V: Fibrinolytic Dysfunction
Clot quality:Clot structure and local [thrombin] Clot strength Low High High Fibrinolysis vulnerability Low Wolberg, AS. Thrombin generation and fibrin clot structure. Blood Review 2007; 21: 131- 142
Colloid solutions (HES) do not activate fibrinolysis, but they do make clots more vulnerable to fibrinolysis
Summary • Variability in hemostasis • One size fits all? • Monitoring • Thrombin generation • Multiple roles • Rate and peak vs. total thrombin • Clot structure • Thrombin • Platelets • Fibrinogen • Clot structure and fibrinolysis