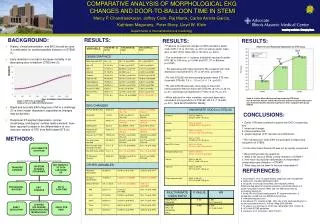
Early Detection of STEMI through EKG Morphology and its Impact on Door-to-Balloon Time
This study analyzes EKG changes in 209 STEMI patients to understand their role in early detection and procedural success. It highlights that the presence of reciprocal changes and the involvement of more ischemic leads correlate with shorter door-to-balloon (DTB) times. Patients presenting with inferior/posterior myocardial infarction showed quicker DTB times. The findings indicate that specific EKG morphologies can enhance early recognition of STEMI, ultimately improving patient outcomes by reducing mortality through faster intervention.

Early Detection of STEMI through EKG Morphology and its Impact on Door-to-Balloon Time
E N D
Presentation Transcript
209 STEMI PATIENTS (FROM EMR) EKG CHANGES EARLY DETECTION? PROCEDURAL SUCCESS Q WAVES STE DEGREE LEADS INVOLVED MORPHOLOGY EKG CHANGES EARLY DTBTIME? ED TO CATH TIME >250 STEMI PTS (2004-2005) TRANSFERPATIENTS 209 STEMI PATIENTS (FROM EMR) NOT DIRECTLY TO CATH LAB FROM ED COMPARATIVE ANALYSIS OF MORPHOLOGICAL EKG CHANGES AND DOOR-TO-BALLOON TIME IN STEMI Mercy P. Chandrasekaran, Jeffrey Cook, Raj Marok, Carlos Arrieta-Garcia, Kathleen Magurany, Peter Stecy, Lloyd W. Klein Departments of Internal Medicine & Cardiology BACKGROUND: RESULTS: RESULTS: RESULTS: • Presence of reciprocal changes on EKG resulted in earlier mean DTB (110 vs 143 mins, p<.001) as well as earlier mean door-to-cath (DTC) times (66 vs 104 mins, p=.0001). • The involvement of >1 ischemic distribution resulted in earlier DTB (82 vs 106 mins, p= 0.046) and DTC (71 vs 88 mins, p=0.0001). • Pts presenting with inferior/posterior MI compared with other distribution had earlier DTC (77 vs 87 mins, p=0.0001). • Pts with DTB<90 min demonstrated greater mean STE than those with DTB>90, 3.0 +/- 1.5 vs 2.4 +/- 1.4, (p<0.01). • Pts with DTB<90 were also more likely to have had inferior/posterior MI than those with DTB>90, (67.2% vs 45.1%, p=.01), and reciprocal depression (71.6% vs 43.7%, p<.01). • When adjusted for other variables, reciprocal depression remained a strong predictor of DTB<90, HR 3.4 (1.76-6.98, p=.001) [SEE MULTIVARIATE TABLE] • History, clinical presentation, and EKG should be used in combination for earliest possible detection of STEMI (1) . • Early detection is crucial to decrease mortality in by decreasing door-to-balloon (DTB) time (2). • Rapid and accurate EKG diagnosis of MI is a challenge (3) is often reader dependent, especially as changes may be dynamic. • Reciprocal ST segment depression, convex morphology, and degree/ number leads elevated, have been reported to assist in the differentiation of non infarction causes of STE from AMI-related STE (4). Graph 2: Inferior MI and Reciprocal Depression by DTB Group Key: Green bars indicate inferior MI, blue dots indicate reciprocal depression and *Asterisk indicates statistical significance when compared with group DTB>90 Graph 1: DTB Time and Mortality Rathore S S et al. BMJ 2009;338:bmj.b1807 CONCLUSIONS: • Earlier DTB were achieved in patient with EKG’s presenting with: • 1. reciprocal changes • 2. inferior/posterior MI • 3. greater degrees of ST elevation and distribution • This indicates that some EKG morphologies increase early recognition of STEMI. • On the other hand, Anterior MI was not as quickly recognized. • These findings raise the questions: • 1. What is the value of EKGs in early detection of STEMI ? • 2. How much do physician deficiencies in interpretation compromise early detection of STEMI? • 3. What steps can be taken to improve interpretation? METHODS: REFERENCES: 1.Braunwald E, et al. Unstable angina: diagnosis and management. 2. Rathore S, et al BMJ 2009;338: b1807 3. Brady WJ et al Acad Emerg Med. 2001 Apr;8(4):349-60. Electrocardiographic ST-segment elevation: correct identification of acute myocardial infarction (AMI) and non-AMI syndromes by emergency physicians. 4. Brady WJ et al Electrocardiographic ST segment elevation: a comparison of AMI and non-AMI ECG syndromes. 5. www.projectupstart.com 6. Zimetbaum PJ, Josephson ME., 935. Use of the electrocardiogram in acute myocardial infarction. N Engl J Med 2003;348:934 7. IC Rokos et al Am Heart J. 2010 Dec;160(6):995-1003, 1003.e1-8 8. ACC/AHA STEMI guidelines 9. Jacobs A, et al. Circulation. 2007;116:217.