Download
1 / 16
160 likes | 289 Views
This study analyzes the outcomes of inappropriate empirical antimicrobial treatment in adult patients with coagulase-negative staphylococcal (CoNS) bacteraemia. A retrospective cohort study was conducted from 2010-2013, involving 98 patients with true CoNS bacteraemia based on clinical presentation. The analysis included 30 cases with appropriate treatment and 68 controls with inappropriate treatment, matched for various factors. Results indicated that initial inappropriate treatment did not significantly affect 30-day mortality among patients with CoNS bacteraemia.

E N D
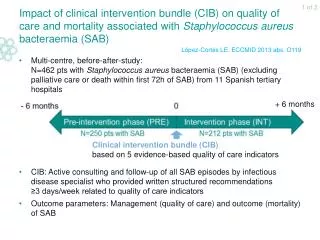
1 of 2 Inappropriate empirical antimicrobial Tx for coagulase-negative staphylococcal (CoNS) bacteraemia: impact on survival Single-centreretrospective cohort study + matched case-control study(South Korea, 2010-2013) N=98 adult patientswithtrueCoNSbacteraemia(≥2 blood cultures positiveforCoNSbased on clinicalpresentation without apparent infection at another site): AppropriateempiricalantimicrobialTx(Txgiven iv ≤48h afterbacteraemiaonset, including ≥1 antibiotictowhichisolate was susceptible): N=30 (‘cases’) InappropriateempiricalantimicrobialTx(includingTxnotadministered≤48h afterbacteraemiaonset): N=68 (‘controls’) Cases andcontrolsmatchedforage, severity of underlyingillness, classification of mainunderlyingdiseases, prior hospitalstay, severity of sepsis, place of infectionacquisition Park S. ECCMID 2014 abs. eP220 Data from poster
2 of 2 Inappropriate empirical antimicrobial Tx for coagulase-negative staphylococcal (CoNS) bacteraemia: impact on survival • Independent predictors of 30-day mortality(cohort study; multivariate analysis): Initial inappropriate antimicrobial Tx does not seem to increase mortality in pts with CoNS bacteraemia Park S. ECCMID 2014 abs. eP220 Data from poster
1 of 2 Fluconazole vs echinocandin/amphotericin B for initial Tx of Candida glabrata bloodstream infection (BSI): efficacy Multi-centre, population-based, observational study (Spain; 2010-2011): N=752 episodes of candidaemia in pts >16 yr N=96 (12.8%) episodes caused by C. glabrata (mixed candidaemia excluded) Annual C. glabrata incidence: 0.53 cases/103 admissions 0.87/104 patient-days N=41 pts received antifungal Tx with fluconazole (FLC) or echinocandin/ amphotericin B (EC/AmB) within first 48h after collection of blood culture (excluding pts dying within first 48h, receiving delayed Tx or other antifungal agents) Fluconazole MIC50/MIC90 of Candida isolates (at 24h): 2/16 (EUCAST) Prior antifungal Tx: 25% of cases; for median time of 8.5 days Puig-Asensio M. ECCMID 2014 abs. eP352 Data from poster
2 of 2 Fluconazole vs echinocandin/amphotericin B for initial Tx of Candida glabrata bloodstream infection (BSI): efficacy • Echinocandin/amphotericin B group: pts more severely ill: *Pos. blood culture after ≥3 days of antifungalTx Early mortality seems not to be affected by the use of fluconazole as initial Tx for C. glabrata BSIs Puig-Asensio M. ECCMID 2014 abs. eP352 Data from poster
1 of 3 Fluconazole vs echinocandins for persistent candidaemia: mycological and clinical outcomes Single-centre retrospective analysis (Taiwan; 2011-2013): N=139 pts ≥18 yr with persistent candidaemia (i.e. persistence of the same Candida species ≥2 days after initiation of antifungal Tx) (only 1st candidaemia episode considered; mixed candidaemia excluded) Incidence of persistent candidaemia: 139/510 candidaemia episodes = 27.3% Eradication rate (i.e. no Candida species isolated from subsequent blood cultures): 48.9% Lin KY. ECCMID 2014 abs. O237 Data fromoralpresentation
2 of 3 Fluconazole vs echinocandins for persistent candidaemia: mycological and clinical outcomes Mycological outcome: median duration of persistence: 7 days Clinical outcome: 14-day mortality rate: 28.8% Lin KY. ECCMID 2014 abs. O237 Data from oral presentation
3 of 3 Fluconazole vs echinocandins for persistent candidaemia: mycological and clinical outcomes Multivariate analysis: NS: not significant Compared with fluconazole, echinocandins did not significantly improve eradication or 14-day mortality in pts with persistent candidaemia. Catheter removal and disease severity, but not echinocandin use, may predict lower mortality Lin KY. ECCMID 2014 abs. O237 Data from oral presentation
1 of 2 Candidaemia: epidemiology, species distribution, antifungal susceptibility and outcome Multi-centre study (2008-2010; pts included in database and prospectively followed; 5 tertiary teaching hospitals in Italy and Spain) N=995 episodes of candidaemia (only 1st episode per patient recorded) Overall candidaemia incidence: 1.55 cases/1,000 admissions; incidence remained stable during period 2008-2010 Mean age: 66.2 yr; 57% males ≥1 comorbidity at time of candidaemia diagnosis: 93.1% of pts Bassetti M et al. J Clin Microbiol 2013;51:4167-72
2 of 2 Candidaemia: epidemiology, species distribution, antifungal susceptibility and outcome • In vitro susceptibility to antifungal agents (CLSI breakpoints): • Lowest MICs: amphotericin B Almost 50% of candidaemia cases were found in IM wards. 30-day mortality rates were higher in HO and IM wards than in other wards Bassetti M et al. J Clin Microbiol 2013;51:4167-72
1 of 2 Combination Tx vs monotherapy for bloodstream infections (BSIs) caused by carbapenemase-producing Klebsiella pneumoniae (CP-Kp): impact on mortality 2-centre, retrospective, observational study (2009-2010; CP-Kp high-prevalence area, Greece): N=205 pts with CP-Kp BSI:VIM (zinc-dependent metallo-β-lactamase): 20.5% − KPC or KPC+VIM: 79.5% All-cause 28-day mortality: 40% (18 pts died ≤48h after bacteraemia onset) Daikos GL et al. Antimicrob Agents Chemother 2014;58:2322-8 †Carbapenem + tigecyclineand/or aminoglycoside and/or colistin *8 ptsinfectedwith pan-resistantK. pneumoniae
2 of 2 Combination Tx vs monotherapy for bloodstream infections (BSIs) caused by carbapenemase-producing Klebsiella pneumoniae (CP-Kp): impact on mortality Independent predictors of 28-day mortality (Cox proportional hazards model; N=175): Compared with monoTx, combiTx may improve survival after CP-Kp BSI, mostly due to the efficacy of carbapenem-containing regimens Daikos GL et al. Antimicrob Agents Chemother 2014;58:2322-8
1 of 2 Adequate monotherapy vs combination Tx for P. aeruginosa (PA) bloodstream infections (BSIs): impact on mortality Post-hoc analysis of multi-centre, prospective cohort study* (Spain; 2008-2009): N=593 pts with single episode of monomicrobial PA BSI (MDR: 22%) 30-day mortality: 30% / Mortality within first 48h: 13% Unadjusted 30-day survival (crude analysis): Peña C et al. Clin Infect Dis 2013;57:208-16 *Peña et al. Antimicrob Agents Chemother 2012;56:1256-72
2 of 2 Adequate monotherapy vs combination Tx for P. aeruginosa (PA) bloodstream infections (BSIs): impact on mortality Multivariate analysis (Cox regression analysis, adjusted for high-risk bacteraemia, Pitt score, shock/multi-organ dysfunction at 48h, PA susceptibility): Combination antimicrobial Tx may not reduce mortality risk compared with monotherapy in PA BSIs Peña C et al. Clin Infect Dis 2013;57:208-16
1 of 3 Albumin + crystalloids vs crystalloids alone in pts with severe sepsis: impact on mortality AlbuminItalianOutcome Sepsis (ALBIOS): multi-centre, open-label, RCT (100 ICUs, Italy; 2008-2012): N=1,818 adult ptswith severe sepsis: Group 1: Crystalloid solution (administeredwheneverclinicallyindicated): N=907 Group 2: Crystalloid solution + 20% albumin (dailyadministrationtomaintain target serum albuminconc. ≥30 g/l): N=903 untildischarge fromICU or 28 daysafterrandomisation Day 1-7: Total dailyamount of administeredfluid: Group 2 ≈ group 1: P=0.10 Mean arterial pressure: Group 2 > group 1: P=0.03 Heartrate: Group 2 < group 1: P=0.002 Daily net fluidbalance: Albumin < crystalloids: P<0.001 Caironi P et al. N Engl J Med 2014;370:1412-21
2 of 3 Albumin + crystalloids vs crystalloids alone in pts with severe sepsis: impact on mortality Mortality Length of stay (secondary endpoint) Caironi P et al. N Engl J Med 2014;370:1412-21
3 of 3 Albumin + crystalloids vs crystalloids alone in pts with severe sepsis: impact on mortality New organ failure (secondary endpoint) SOFA (sub)score (secondary endpoint) In pts with severe sepsis, addition of albumin to crystalloids does not seem to improve survival after 28 and 90 days Caironi P et al. N Engl J Med 2014;370:1412-21