Download
1 / 12
120 likes | 254 Views
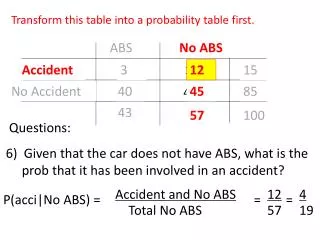
1 of 2. Value of rapid antigen detection tests (RADTs) for diagnosis of invasive group A Streptococci ( GAS). 3-centre, retrospective study: N=192 miscellaneous clinical samples (pleural and synovial fluids, subcutaneous, gynaecological/digestive abscesses,...):

E N D
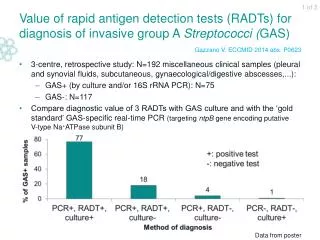
1 of 2 Value of rapid antigen detection tests (RADTs) for diagnosis of invasive group A Streptococci(GAS) 3-centre, retrospective study: N=192 miscellaneous clinical samples (pleural and synovial fluids, subcutaneous, gynaecological/digestive abscesses,...): GAS+ (by culture and/or 16S rRNA PCR): N=75 GAS-: N=117 Compare diagnostic value of 3 RADTs with GAS culture and with the ‘gold standard’ GAS-specific real-time PCR (targeting ntpB gene encoding putative V-type Na+ATPase subunit B) Gazzano V. ECCMID 2014 abs. P0623 Data from poster
2 of 2 Value of rapid antigen detection tests (RADTs) for diagnosis of invasive group A Streptococci(GAS) The 3 RADTs showed a higher sensitivity than GAS culture, but were less sensitive than GAS-specific PCR. They may be used to speed up diagnosis when invasive GAS infections are suspected Gazzano V. ECCMID 2014 abs. P0623 Data from poster
1 of 2 Unique blood culture (UBC) vs multiple blood culture (MBC): diagnostic performance 1-yr, multi-centre, prospective study (France): N=826 pts ≥18 yr admitted to adult ICU with fever ≥38.5°C, hypothermia ≤36.0°C, chills or shock N=300 pts with positive BC (mean age: 67.3 yr): Pathogens: N=245 / Contaminants: N=55 Dargere S. ECCMID 2014 abs. P0484 Data from poster
2 of 2 Unique blood culture (UBC) vs multiple blood culture (MBC): diagnostic performance • Discrepancies: • MBC vs UBC (1 centre): cost savings: 193,275 €/yr (materials, labour time) UBC may decrease the # of false positives and false negatives compared with MBC and may lead to significant cost savings Dargere S. ECCMID 2014 abs. P0484 Data from poster
2 of 2 Unique blood culture (UBC) vs multiple blood culture (MBC): diagnostic performance • MBC vs UBC (1 centre): cost savings: 193,275 €/yr (materials, labour time) UBC may decrease the # of false positives and false negatives compared with MBC and may lead to significant cost savings Dargere S. ECCMID 2014 abs. P0484 Data from poster
1 of 2 MALDI-TOF for pathogen identification in blood cultures (BCs): improved methods Short-incubation (SI) MALDI-TOF forrapidpathogen identification1: 3-centre study (Finland): 50-100 ml bloodfrom pos. BC bottleaspiratedontoblood, chocolate and FAA agarplates → incubation 3-4h 37°C CO2atmosphere Sample fromapplication area of eachplate spread on a MALDI-TOF target plate, even if no visiblegrowth+ 1 µl matrix suspension added + air drying → samples analysed in MALDI-TOF instruments Comparisonwithconventional MALDI-TOF or otheridentificationmethods 1Kalanti A. ECCMID 2014 abs. P0495 2Østergaard C. ECCMID 2014 abs. P0494 Data from poster
2 of 2 MALDI-TOF for pathogen identification in blood cultures (BCs): improved methods MALDI-TOF-MS directly on positive BCs2: Single-centrestudy (2013-2014; Denmark): N=1,068 uniqueisolates • 2 ml bloodfrom pos. BC bottlecentrifuged (1,000g; 2 min) toremoveRBCs → supernatantcentrifuged (14,000g; 10 min) → bacteria in pellet • Sample from pellet transferredto MALDI-TOF target plate, without proteinextraction+ standard matrix added → analysed in MALDI-TOF instrument • Comparisonwithconventional MALDI-TOF (samples cultured on 5% Danishbloodor anaerobicagarplates) (cut-off score: 1.7) Short-incubation MALDI-TOF or MALDI-TOF directly on pos. BC bottles may simplify and fasten pathogen identification in BCs 1Kalanti A. ECCMID 2014 abs. P0495 2Østergaard C. ECCMID 2014 abs. P0494 Data from poster
1 of 2 MALDI-TOF + antimicrobial stewardship team (AST) intervention: impact on outcomes in pts with bloodstream infections (BSIs) Single-centre before-after study (USA): N=501 adult pts with BSI Pre-intervention phase (Sep-Nov 2011): BSI identified by conventional methods Intervention phase (Sep-Nov 2012): BSI identified via MALDI-TOF + real-time evidence-based antibiotic recommendations by AST Huang AM et al. Clin Infect Dis 2013;57:1237-45
2 of 2 MALDI-TOF + antimicrobial stewardship team (AST) intervention: impact on outcomes in pts with bloodstream infections (BSIs) • Multivariate analysis for predictors of mortality: Acceptance of AST intervention: trend towards reduced mortality: OR=0.55; 95% CI:0.28-1.06; P=0.075 MALDI-TOF + AST intervention may decrease time to organism identification and time to effective and optimal antibiotic therapy Huang AM et al. Clin Infect Dis 2013;57:1237-45
1 of 3 1,3-β-D-glucan (BG) antigenaemia: accuracy for diagnosing intraabdominal candidiasis (IAC) Fungal Infection Network of Switzerland (FUNGINOS): 2-centre, prospective, observational cohort study (2007-2010): median FU: 19 days N=89 adult ICU pts (≥72h in ICU) with recurrent GI tract perforation (N=68) or acute necrotising pancreatitis (N=21); 920 sera analysed (9 sera/patient) Tissot F et al. Am J Respir Crit Care Med 2013;188:1100-9
2 of 3 1,3-β-D-glucan (BG) antigenaemia: accuracy for diagnosing intraabdominal candidiasis (IAC) Mortality/sepsis rate among pts with documented IAC (N=29): Time between microbiological diagnosis of IAC (day 0) and time of reaching value above the cut-off value (per diagnostic method): Tissot F et al. Am J Respir Crit Care Med 2013;188:1100-9
3 of 3 1,3-β-D-glucan (BG) antigenaemia: accuracy for diagnosing intraabdominal candidiasis (IAC) Accuracy (N=29 pts with documented IAC; maximum value up to time of IAC diagnosis compared with day 7 after inclusion in pts without IAC) *Accuracy=(true positives + true negatives)/ all results; †2 consecutive BG measurements; (C)CI: (corrected) Candida colonisation index; CS: Candida score; NPV: neg. predictive value; PPV: pos. predictive value In high-risk surgical ICU pts, BG antigenaemia was more accurate than CS and (C)CI and anticipated diagnosis of blood culture-neg. IAC Tissot F et al. Am J Respir Crit Care Med 2013;188:1100-9