Download

1 / 42
560 likes | 1.09k Views
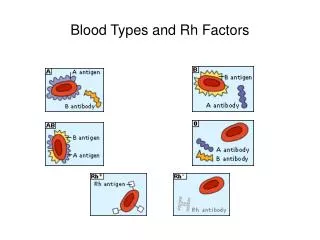
Rh Blood Group System. Objectives. Name the common antigens associated with the Rh system Recognize other Rh antigens Recognize the three terminologies of the Rh Blood Group System Discuss the reactivity, thermal range, incidence, inheritance and clinical importance of the Rh antigens

E N D
Objectives • Name the common antigens associated with the Rh system • Recognize other Rh antigens • Recognize the three terminologies of the Rh Blood Group System • Discuss the reactivity, thermal range, incidence, inheritance and clinical importance of the Rh antigens • Discuss the significance of a weak D
Objectives (cont) • Explain the relationship between weak D testing in the mother and fetal maternal hemorrhage • Discuss LW, G, f, Null phenotype • Understand the clinical significance of associated antibodies to the Rh Blood Group System • List and explain the reasons for a positive Rh control • Given the results of routine Rh testing, identify the problem and describe an appropriate solution
Rh Blood Group System • 45 antigens identified • Encoded on chromosome 1 • RHD, RHCE (genes) • RhD polypeptide, RhCE polypeptide (products) • Possible involvement in RBC membrane integrity • Rh Null individuals have stomatocytosis
Biochemistry (cont) • Non-glycosylated protein (no carbohydtates attached) • RHD and RHCE gene encode proteins remarkbly similar • 417 amino acids • Traverse the membrane 12x • Differ by 44 base pairs • C/c differ by 4 amino acidsand E/e differ by 1 amino acid
Rh Terminology • Fisher-Race • Each antigen and corresponding gene given the same letter designation (D, C, E, c, e) • Phenotype is defined by the presence of the D, d, C, E, c, and e expression • Co-dominance expression…both a C and a c can be expressed • Example; DCE/dCe
WeinerTerminolgy • Gene responsible for defining Rh produced an agglutinogen containing a series of factors • The upper case R denote the presence of D • The presence of C is denoted by a 1 or a ‘ • The presence of E is denoted by a 2 or a ‘’ • Lower case c is imlied when there is no 1 or ‘ • Lower case e is implied when there is no 2 or ‘’ • Example-Rh0=Rh0=Rh0hr’hr’’ R0(Dce in Fisher-Race)
RosenfieldTerminology • Assigns a number to each antigen of the Rh system • Easier as more and more antigens were identified in the Rh system. • No genetic basis • A minus sign preceding the number signifies the absence of the antigen • Example: 1, -2, -3, 4, 5 (Dce/Dce in Fisher race)
ISBT Terminolgy • International Universal language • Six digit number for each blood group specificity • First three numbers represent the sytem (Rh) and the last three represent the antigenic specificity • Example: D= 004001
Overview of Rh Terminologies • Tables 7–2, 7–3, and 7–4 summarize the data presented in this section. • Table 7–5 correlates Rh phenotypes with the most probable or predicted genotype in a designated population.
Overview of Rh Terminologies (cont’d) • RHD and RHCE, all upper case and in italics indicate genes. • RhD, RhCe, RhcE, Rhce, and RhCE designate proteins on which the Rh antigens reside.
RH Genes • Tippettproposed that two closely linked genes, RHD and RHCE located on chromosome 1 control expression of Rh proteins;. • The gene RHD codes for the presence or absence of the RhD protein. • The gene RHCE codes for either RhCe, RhcE, Rhce, or RhCEpolypeptides.
RH Genes (cont’d) • Another gene important to Rh antigen expression is RHAG on chromosome 6. • The product of this gene is Rh-associated glycoprotein (RhAG). • RhAG is termed a coexpressor and must be present for successful expression of the Rh antigens.
Rh-Positive Phenotypes • Rh-positive individuals inherit one or two codominant RHD genes, which result in expression of RhD antigen and are typed Rh-positive. • In addition to the RHD gene(s), two RHCE genes are inherited, one from each parent.
Rh-Negative Phenotypes • Rh-negative individuals can arise from at least three different mutations. • These mutations are most often found in individuals falling into three different ethnic backgrounds. • European ethnicity • African ethnicity • Asian ethnicity
RhAG • RhAG does not express any Rh antigens. But: • When mutations in the RHAG gene occur, it can result in missing or significantly altered RhD and RhCE proteins, affecting antigen expression. • Rhnull phenotype
Weak D: Variations of D Antigen Expression • Some RBCs possess weaker expression of D antigen that requires an indirect antiglobulin test to detect the D antigen. • Individuals with altered D antigen are categorized into different phenotypes defined as weakened D. • C in trans to RHD • Weak D • Partial D • Del
C in Trans to RHD • When Ce (r’) is present in trans to RHD (example: Ror’ • The expression of D is depressed
Weak D • Various types of phenotypes in which there is a reduced amount of D antigen sites • Usually results from a single nucleotide mutation in RHD • IAT techniques needed to detect the presence of the D antigen (weak D testing)
Partial D • Individuals who are D+ that make anti-D • Occurrence of hybrid genes in which portions of RHD is replaced by RHCE • Results in a loss od D epitopes
Del • D antigen is not detected by routine methods • Absorption/elution techniques using anti-D prove the existance of a D antigen • Occur in Asian population
Detection of Rh Antibodies and Antigens • Most Rh antibodies are IgG and react optimally at 37°C or after AHG testing. • Rh antibodies are usually produced following exposure to foreign RBCs. • Rh antibodies may show dosage. • Rh antibodies are enhanced when testing with enzyme-treated RBCs.
Detection of Rh Antibodies and Antigens (cont’d) • IgG1, IgG2, IgG3, and IgG4 subclasses of Rh antibodies have been reported. • IgG1 and IgG3 are of the greatest clinical significance; RBCs coated with IgG1 and IgG3 are rapidly cleared from the circulation by the RES.
Detection of Rh Antibodies and Antigens (cont’d) • Rh antibodies often persist for years. • Rh antibodies do not bind complement. • Rh antibodies can traverse the placenta.
Rh Typing Reagents • reagent anti-D that allow for typing individuals’ RBCs as quickly and accurately as typing for ABO. • Reagents may be high-protein–based or low-protein–based, saline-based, chemically modified, monoclonal, or blends of monoclonals.
The Landsteiner Weiner (LW) Blood Group System • The LW system dates from the time when Rh antigens were first recognized. • The antibody produced by injecting rhesus monkey RBCs into guinea pigs and rabbits was identified as having the same specificity as the antibody Levine and Stetson described earlier.
The Landsteiner Weiner (LW) Blood Group System (cont’d) • Many years later, it was recognized that the two antibodies were not identical; the anti-rhesus described by Landsteiner and Wiener was renamed anti-LW in their honor. • Phenotypically, there is a similarity between the Rh and LW systems.
The Landsteiner Weiner (LW) Blood Group System (cont’d) • Anti-LW reacts strongly with most D-positive RBCs, weakly (sometimes not at all) with Rh-negative RBCs, and never with Rhnull cells. • Anti-LW usually shows stronger positive reactions with D-positive RBCs than with D-negative adult RBCs. • Anti-LW reacts equally well with cord cells regardless of their D type.
Cw • Altered C antigen • European descent
G antigen • Located on red cells possessing D or C • Antibody appears to be anti-D plus anti-C but cannot be separated • Absorbed by D-C+ or D+C-
f antigen • Compound antigen • ce
Ce • Compound antigen • Located on R1 (Dce) or r’ (Ce)
Rh Null • Rh associated protein, RhAG, encoded by a single gene on chromosome 6 • Associated with Rh antigens to form Rh-core complex • Rh null individuals lack all Rh antigens • Phenotype results from mutations in RhAG which results in no expression if Rh antigens on red cells
Clinical Considerations: Transfusion Reactions • The D antigen is the most immunogenic antigen outside the ABO system. • Careful review of the medical history for pregnancy or transfusion of products containing RBCs • Unexplained fever, a mild bilirubin elevation, and a decrease in hemoglobin and haptoglobin • The DAT is usually positive • Antibody screen may demonstrate circulating antibody • Elution studies may be helpful
Hemolytic Disease of the Fetus and Newborn • HDFN caused by Rh antibodies is often severe; the Rh antigens are well developed on fetal cells, and Rh antibodies are transplacentalIgG. • Rh-immune globulin, a purified preparation of IgG anti-D, is given to D-negative woman during pregnancy and after delivery of a D-positive fetus. • Rh-immune globulin is effective only in preventing RhDHDFN.
Rh Deficiency Syndrome: Rhnull and Rhmod • Individuals who lack all Rh antigens on their RBCs are said to have Rhnull syndrome • Individuals of the Rhmod phenotype have a partial suppression of RH gene expression caused by mutations in the RHAG gene • When the resultant RhAG protein is altered, normal Rh antigens are also altered often causing weakened expression of the normal Rh and LW antigens
Reagents • Early reagents were polyclonal and IgG, recognize many epitopes • High-protien additives were added to enhance potency, but resulted in spontaneous agglutination • Monoclonal reagents were developed in the 1980s that reacted to single D epitopes but did not detect all D positive cells • Most reagents now are monoclonal blends of varying clones