Download
1 / 41
490 likes | 1.86k Views
The Rh Blood Group. Brian Poirier, MD UCDavis Medical Center. Topics. Terminology systems Rh antibodies Consequences of Rh incompatibility Unusual phenotypes. Objectives. Explain the derivation of the term Rh Differentiate Rh from LW

E N D
The Rh Blood Group Brian Poirier, MD UCDavis Medical Center
Topics Terminology systems Rh antibodies Consequences of Rh incompatibility Unusual phenotypes
Objectives Explain the derivation of the term Rh Differentiate Rh from LW Compare and convert the major genotypes among Fisher-Race, Wiener, and Rosenfield terminologies Define the basic biochemical structure of Rh
Objectives (Continued) Describe and differentiate three mechanisms that result in weak D expression on rbcs Describe 3 characteristics of Rh antibodies Describe how to prevent Rh D immunization
Rh Blood Group Second most important blood group (after ABO)
History of the Rh System • 1939 Levine described a HTR in an OB patient: • After delivery of a still born infant, a woman required transfusions. • After receiving her husband’s blood (ABO compatible), she demonstrated the acute HTR. • An antibody was isolated from mom’s serum that reacted both at 37 C and 20 C with father’s rbcs.
History of the Rh System (continued) • 1940 Landsteiner and Wiener reported: • An antibody made by guinea pigs and rabbits when they were transfused with rhesus monkey rbcs. • The antibody agglutinated 85% of human rbcs, was named “Rh.” • The antibody was renamed as anti-LW (Landsteiner and Wiener). • The name Rh was retained for human-produced antibody.
Nomenclatures of the Rh system Fisher-Race: The DCE Terminology Wiener (Rh-Hr): The Rh-Hr Terminology Rosenfield: Alpha/Numeric Terminology ISBT (International Society of Blood Transfusion): Numeric Terminology
Fisher-Race (DCE or CDE) • 5 major antigens: D, C, E, c, e • Rh positive really means D positive. • Absence of D designated “d” (later found not to be a real antigen- an “amorph”). • 8 potential haplotypes named based on presence of genes for above antigens (eg, Dce, dce).
Wiener (Rh-Hr) • Different names for the 5 main antigens • Rho=D • rh’=C • rh”=E • hr’=c • hr”=e
Wiener (Rh-Hr) (continued) • Gave shorthand names to the 8 potential combinations alluded to above; still in use R1=DCe r’=dCe R2=DcE r”=dcE Ro=Dce r=dce Rz=DCE ry=dCE
Converting Wiener (Rh-Hr) to Fisher-Race Fisher-Race terminology is easier to use: • R=D, r=d • 1 or prime=C • 2 or double prime=E • 0 or blank=ce • any superscript letter =CE
Rosenfield Terminology (alpha/numeric) Rosenfield system has no genetic basis, only demonstrates the presence or absence of the antigen on the red cells. A minus sign preceding a number designates absence of the antigen. The absence of the number indicates the antigen has not been typed.
Rosenfield Terminology (Continued) D is assigned Rh1; C is assigned Rh2; E is assigned Rh3; c is assigned Rh4; e is assigned Rh5 Example 1: D+ C- E+ c+ e+ would be: Rh: 1, -2, 3, 4, 5 Example 2: DCe/dcE would be: Rh: 1, 2, 3, 4, 5
ISBT Terminology ISBT adopted a six-digit number for each blood goup specificiy. First 3 numbers represent the system and the remaining 3 the antigen specificity. 004 was assigned to the Rh blood group system; each antigen assigned to the Rh system was given a unique number to complete the 6-digit computer number. Example: “D” antigen would be “004001”
“The Big Four Rh Phenotypes R1, R2, R0, and r are most frequently encountered phenotypes. R0 most common in blacks, least common in whites. R1> R2 r is always second in frequency Whites: R1 > r > R2 > R0 Blacks: R0 > r > R1 > R2
Gene Frequency of Rh Antigens GeneFrequency % D 85 d 15 C 70 E 30 c 80 e 98
Common Rh Types by 3 Nomenclatures Wiener Fisher-Race Rosenfield % R1r DCe/dce Rh: 1,2,-3, 4,5 33 R1R1 DCe/DCe Rh: 1,2,-3, -4,5 18 rr dce/dce Rh: -1,-2,-3, 4,5 15 R1R2 DCe/DcE Rh: 1,2,3, 4,5 11 R2r DcE/dce Rh: 1,-2,3, 4,5 9 R2R2 DcE/DcE Rh: 1,-2,3, 4,-5 2
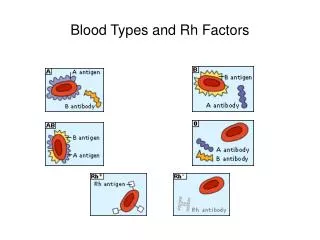
Rh Antigens Non-glycosylated proteins in the red cell membrane. Inherited as codominant alleles. Are transmembrane polypeptides and are an integral part of the red cell membrane. All Rh antigens (D,C,E) are very similar; differ by only 44 base pair. C and c differ in 4 a.a. E and e differ in 1 a.a.
Rh Antigens Hillyer et al 2009
Rh Antigens (continued) • Rh antigens are highly immunogenic: D > c > E > C > e • The D antigen is the most immunogenic antigen outside the ABO system. • As little as 0.5 ml will elicit anti-D allo-immunization in healthy volunteers (Gunson et al 1970).
Rh Antibodies Do not bind complement Extravascular IgG Can cross placenta and cause HDFN HTR Exposure required (pregnancy or transfusion)
Consequences of Rh Incompatibility Unexposed: 80% of healthy D negative individuals make anti-D with one unit transfused. Approximately 22% of hospitalized (non-oncology) patients (Yazer et al 2007). Exposed: HTRs with extravascular hemolysis Most severe HDFN
Prevention of D Immunization:RhIgG Macro dose (300 g): protect against 30 mL of WB or 15 mL of packed RBCs Micro dose (50 g): protect against 5 mL of WB; sufficient for abortion, amniocentesis, and ectopic rupture at up to 12 weeks gestation
Unusual Rh Phenotypes Weak D phenotype Du Rhnull phenotype Compound Rh antigens
Weak D phenotype (Du) • Some D positive individuals require AHG phase to demonstrate D antigen • Reasons: • C opposite chromosome to D (C in trans position): eg, Dce/dCe • Genetic weak D (weakened D expression) • Partial D (“Mosaic”) • (most prone to making anti-D)
Determination of D Status Donors: D neg donors must be confirmed by AHG test Recipients: D neg recipients do not need to be confirmed by AHG (though most are)
Rh antigen typing reagents Saline anti-D (IgM, can’t be used for Du) High protein anti-D (requiring Rh control) Chemically modified anti-D (low protein) Monoclonal anti-D Blend of Monoclonals (anti-IgM and anti-IgG anti-D)
Rhnull Phenotype Lacks all Rh antigens Rhnull syndrome demonstrates a mild compensated hemolytic anemia with stomatocytosis, spherocytosis and reticulocytosis Transfuse with Rhnull blood The clinical symptoms of Rhmod phenotype are less severe and rarely clinically remarkable.
Compound Rh Antigens f = antigen present when c and e are on the same chromosome G: G is present on most D pos and all C pos RBCs. Anti-G originally appeared to be anti-D+C; further investigation showed that anti-G was directed toward D+G.
The LW System LW antigens Anti- LW
LW Antigens (normal pathway) Precursor substance ÜDCE genes normal Rh antigens LWa LWb genesßà LW genes LW pos LW neg
Anti- LW: • Reacts strongly with most D pos rbcs. • Reacts weakly with D neg rbcs. • No reaction with Rhnull rbcs. • Reacts equally well with cord cells regardless of D typing. • Rarely clinically significant.
Objectives Explain the derivation of the term Rh Differentiate Rh from LW Compare and convert the major genotypes among Fisher-Race, Wiener, and Rosenfield terminologies Define the basic biochemical structure of Rh
Objectives (Continued) Describe and differentiate three mechanisms that result in weak D expression on rbcs Describe 3 characteristics of Rh antibodies Describe how to prevent Rh D immunization
THANKS TO Rosemary Howard, CLS Dr Chris Gresens
References • Transfusion Medicine and Hemostasis, Hillyer et al, 2009, Elsevier Pub. • Yazer et al, (2007), Detection of anti-D in D- recipients transfused with D + red cells, Transfusion 47 2197-2201 • Avent ND, Reid (2000) The Rh blood group system: a review Blood 95 375-387. • Gunson et al (1970) The Anti-Rh0(D) Responses of Immunized Volunteers following Repeated Antigenic Stimuli, BJH