Download
1 / 16
190 likes | 469 Views
Diseases of adrenal cortex & medulla. Ali Al Khader, M.D. Faculty of Medicine Al-Balqa’ Applied University Email: ali.alkhader@bau.edu.jo. Lecture outline. Adrenocortical hyperfunction (Hyperadrenalism): -Hypercortisolism (Cushing syndrome) -Primary hyperaldosteronism

E N D
Diseases of adrenal cortex & medulla Ali Al Khader, M.D. Faculty of Medicine Al-Balqa’ Applied University Email: ali.alkhader@bau.edu.jo
Lecture outline • Adrenocortical hyperfunction (Hyperadrenalism): -Hypercortisolism (Cushing syndrome) -Primary hyperaldosteronism -Adrenogenital (virilizing) syndromes…excess androgens • Adrenocortical insufficiency • Adrenocortical neoplasms • Tumors of the adrenal medulla: -Pheochromocytoma -Neuroblastoma
Hypercortisolism (Cushing syndrome) Exogenous (Iatrogenic) Endogenous -Thinning of hair -Acne -Red cheeks -Moon face -Supraclavicular fat pad -Increased body and facial hair -Hypertension -Diabetes -Immunodeficiency -Weight gain -Purple striae -Pendulous abdomen -Thin extremities with muscle atrophy -Ecchymosis resulting from easy bruising -Menstrual abnormality -Thin skin and subcutaneous tissue -Slow wound healing -Mental/psychological manifestations The most common Elsevier. Kumar et al. Robbins and Cotran pathologic basis of diseases 9th…Reproduced with permission from Lloyd RV, et al (eds): Atlas of Nontumor Pathology: Endocrine Diseases. Washington, DC, American Registry of Pathology, 2002.) ACTH-independent ACTH-dependent Less common than -Adrenal adenoma -Adrenal carcinoma -Hyperplasia (a subset of them is seen in McCune-Albright syndrome (GNAS mutations)) Ectopic ACTH …e.g., lung small cell carcinoma -Pituitary tumor (mostly ACTH-secreting microadenoma) -Rarely: increased CRH (from hypothalamus) Middle-aged males more Young adult females more = Cushing disease
Cushing syndrome, laboratory diagnosis Cushing disease Ectopic ACTH Adrenal tumor -ACTH is not suppressed with low-dose dexamethasone …urinary steroid secretion is not decreased -ACTH is suppressed with high-dose dexamethasone …urinary steroid secretion is decreased No response to high- or low-dose dexamethasone ACTH is already low and cortisol excretion is not affected by low- or high-dose dexamethasone
The most common cause of 2ry hypertension Primary hyperaldosteronism • Autonomous overproduction of aldosterone, with resultant suppression of the renin-angiotensin system and decreased plasma renin activity • Causes: Bilateral idiopathic hyperaldosteronism…the most common Bilateral nodular hyperplasia Adenoma (Conn syndrome) or carcinoma Older age & less severe hypertension than hyperaldosteronism due to adrenal tumor Middle-aged women more 2ry Hyperaldosteronism: …in response to activation of the renin-angiotensin system …characterized by increased levels of plasma renin …seen in conditions of decreased renal perfusion
Primary hyperaldosteronism, clinical features & diagnosis • Hypertension with resulting left ventricular hypertrophy and cardiovascular compromise, strokes & MIs • Hypokalemia (weakness, paresthesias, visual disturbances, and occasionally frank tetany) • Elevated plasma aldosterone to renin ratio …if this screening test is positive, a confirmatory aldosterone suppression test (by salt or captopril for example) must be performed …if the aldosterone levels are still high and the renin levels are still low after the suppression test, the diagnosis is confirmed
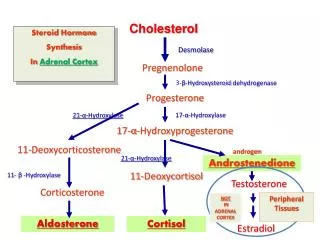
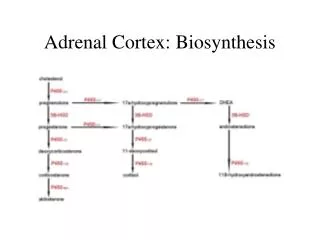
Adrenogenital (virilizing) syndromes Adrenocortical neoplasms Congenital adrenal hyperplasia (CAH) Carcinomas more than adenomas The mostcommon enzymatic defect in CAH is 21-hydroxylase deficiency…a spectrum of severity depending on the mutation 21-hydroxylase is required for synthesis of cortisoland aldosterone but not sex steroids Cortisol is not synthesized (&/or aldosterone) In response to ACTH, no cortisol will be synthesized but the androgen synthesis pathway will be activated instead ACTH is increased
Adrenogenital (virilizing) syndromes, clinical features • The onset of clinical symptoms may occur in the perinatal period, later childhood, or (less commonly) adulthood • In 21-hydroxylase deficiency: -Masculinization (virilization) in females: -In males: Enlargement of the external genitalia, precocious puberty in young patients. Most men with CAH are fertile but some have failure of Leydig cell development and oligospermia 1/3: aldosterone deficiency and some may have risk for acute adrenal insufficiency Clitoral hypertrophy and pseudohermaphroditismin infants or oligomenorrhea, hirsutism, and acne in postpubertal girls …an ovarian tumor must also be excluded Always rule out CAH in any neonate with ambiguous genitalia
No hyperpigmentation Normal aldosterone Adrenocortical insufficiency Hyperpigmentation Primary Secondary = Adrenal crisis …due to ACTH deficiency = Addison disease Fatigue Vomiting Diarrhea Anorexia, nausea & weight loss Hypoglycemia Hyperkalemia Hyponatremia Hypotension …mainly: lung & breast Elsevier. Kumar et al. Robbins basic pathology 10th…modified
Notes on adrenocortical adenoma and carcinoma • The most common adrenal malignancy is metastases (especially from the lung or breast) • Adenoma is usually nonfunctional and is usually discovered incidentally (incidentaloma) • “Functional” or “nonfunctional” cannot be predicted from morphology • Behavior is more important than morphology to differentiate between adenoma and carcinoma
Pheochromocytoma Catecholamine cardiomyopathy, or catecholamine-inducedmyocardial instability and ventricular arrhythmias and cerebrovascular accidents are serious complications • A tumor of chromaffin cells • A cause of 2ry hypertension…mainly paroxysmal (with palpitations, sweating & tremor) • Rule of 10s: 10% of pheochromocytomas are extraadrenal… = paragangliomas 10% of adrenal pheochromocytomas are bilateral 10% of adrenal pheochromocytomas are malignant 10% of adrenal pheochromocytomas are not associated with hypertension 25% are familial…6 known genes (RET, NF1, VHL, SDHB, SDHC, SDHD) There is usually base-line hypertension Lab results: Increased urinary excretionof free catecholamines and their metabolites, such asvanillylmandelic acid and metanephrines
Pheochromocytoma Capillary network Nest This nested pattern is called: Zellballen pattern Nest Nest Modified from: T Karthikeyan, D Manimaran, V Mrinalini. MulticentricParaganglioma Of The Bladder - A Rare Case Report. The Internet Journal of Pathology. 2012 Volume 13 Number 2. Sustentacular cells
Neuroblastoma • The most common extracranial solid tumor of childhood …most commonly during the first 5 years of life and may arise during infancy • It arises from primordial neural crest cells • Neuroblastomas may occur anywhere in the sympathetic nervous system and occasionally within the brain, but they are most common in the abdomen (esp., adrenal medulla)
Homer Wright rosettes Elsevier. Kumar et al. Robbins and Cotran pathologic basis of diseases 9th
Neuroblastoma Unfortunately, most (60% to 80%) children present with stage 3 or 4 4S tumors have an excellent prognosis withminimal therapy, and it is not uncommon for theprimary or metastatic 4S tumors to undergo spontaneousregression *Age <18 months: favorable prognosis *Certain genetic/chromosomal abnormalities are important in the prognosis (e.g., MYCN oncogene amplification is bad) *Certain histological features are important in the prognosis (Gangliocytic differentiation is associated with favorable prognosis, high mitotic activity is bad) *Stages 1, 2A, 2B & 4S are better than 3 & 4 Elsevier. Kumar et al. Robbins basic pathology 10th…modified