Download
1 / 42
420 likes | 574 Views
This guide reviews the basics of assessing the musculoskeletal system, covering inspection, palpation, movement, stability, and function. It includes GALS recording, tips for specific body parts, and biomechanics insights. Suitable for quick and thorough assessments in general practice.

E N D
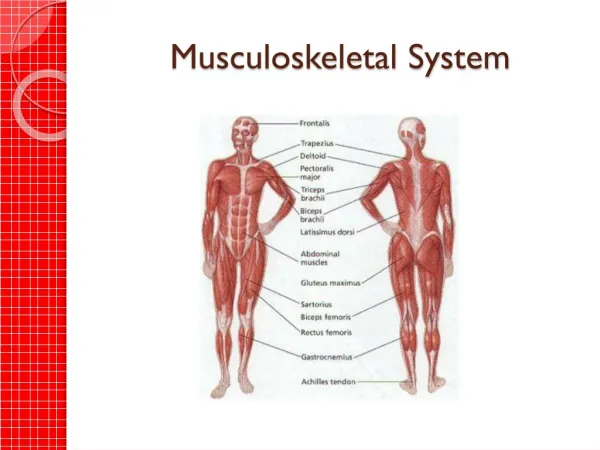
Easy assessment of musculoskeletal system for GPs Aspects of examining the musculoskeletal system
Revisiting the basics • GALS • Video • Some bits and pieces / a personal view
History • “Have you any pain or stiffness in your muscles, joints or back?” • “Do you have any trouble getting up or down stairs?” • “Do you have any difficulty getting dressed?”
Revisiting the basics • Inspection Look • Palpation Feel • Movement Move • Stability • Function • Compare with opposite side
Inspection • Skin colour / rashes • Swelling • Deformity • Scars • Muscle wasting • Surrounding structures - bursae, tendons
Palpation • Nature of swelling • bony • synovial • effusion • Warmth • Tenderness
Movement • Active and passive • Range of movement • Crepitus • Note pain • Instability
Stability • Subluxation or dislocation • MCP • Radioulnar • subtalar • MTP
Function • Lower limbs - gait • Hands • pincer grip • power grip
Doherty, Dacre, Dieppe and Snaith (1992) The GALS locomotor screen, Annals of Rheumatic diseases 51: 1165-9 GAIT ARMS LEGS SPINE G A L S
G A L S • “…provide a valuable screening test for use in general practice” • “the procedure can be viewed as a general functional (disability), as well as a basic musculoskeletal assessment” • “..be useful in selective situations as a rapid test of functional performance and to screen out regional locomotor abnormalities that merit closer scrutiny”
Hands Wrists - CTS + de Q Shoulders Backs Hips Feet - biomechanics Hypermobility Fibromyalgia Bits and pieces
Early synovitis • PIP - skin discolouration and tenderness • Clench fist - MCPs should be white with no infilling • MCP squeeze to elicit tenderness • Inferior radio ulnar stress test • Bulge sign at knee • MTP squeeze test
Carpal Tunnel Syndrome • Phalen’s • Tinel’s
De Quervains tenosynovitis • APL and EPB tendons • tender over radial styloid • sometimes nodule (thickened sheath) • Finkelsteins test • Rest it • Inject it
Shoulders • Shoulder or not • Glenohumeral or not - external rotation • Tenderness • bicipital groove • subacromial • Painful arc of abduction
Backs • Lumbar flexion • Modified Schobers - or use your fingers • Fingers to floor = misleading • Lumbar extension • Lumbar lateral flexion • “Sacroiliac restriction”
Hips • Internal rotation - can examine sitting • Trochanteric bursitis • Trendelenburg - to distinguish lumbosacral from hip pain
Foot - biomechanics • Swing phase • Stance phase • Contact (27%) • Midstance (40%) • Propulsive (33%)
Biomechanics - stance phase • Contact • outer border heel strikes then • PRONATION at subtalar joint shifts centre gravity medially • causes tibia to internally rotate • purpose is shock absorption/adaption uneven ground
Biomechanics - stance phase (2) • Midstance • forefoot loaded • subtalar joint supinates • causes tibia to externally rotate • foot is converted to rigid lever ready for propulsion • ends with heel lift
Biomechanics - stance phase (3) • Propulsion • app 25% bodyweight on metatarsals and toes (esp 1st) • ends with toes off
Subtalar pronation unchecked longitudinal arch stretches and flattens excess rotation of tibia Hallux valgus Plantar fasciitis Achilles tendonitis Post tibial tendonitis stress# navicular anterior knee pain low back pain Over pronation
Hypermobility • Dorsiflexion of 5th MCP to 90 degrees • Apposition of thumb to volar aspect of forearm • Hyperextension of elbow by 10 degrees • Hyperextension of knee by 10 degrees • Hands flat on floor with knees extended