Download
1 / 1
10 likes | 143 Views
BREAST CANCER SCREENING, PREVALENCE AND HEALTHCARE UTILIZATION AND COST TRENDS AMONG FEE-FOR-SERVICE FEMALE RECIPIENTS IN A STATE MEDICAID PROGRAM Khanna R, Madhavan SS, Bhanegaonkar A School of Pharmacy and Mary Babb Randolph Cancer Center, West Virginia University, Morgantown, WV.

E N D
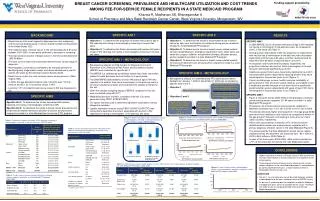
BREAST CANCER SCREENING, PREVALENCE AND HEALTHCARE UTILIZATION AND COST TRENDS AMONG FEE-FOR-SERVICE FEMALE RECIPIENTS IN A STATE MEDICAID PROGRAM KhannaR, MadhavanSS, BhanegaonkarA School of Pharmacy and Mary Babb Randolph Cancer Center, West Virginia University, Morgantown, WV SPECIFIC AIM 2 SPECIFIC AIM 1 • Objective 1: To determine the trends in the prevalence rate of breast cancer by age, race, and location of residence among women recipients enrolled in a state Medicaid FFS program. • Objective 2: To determine the trends in breast-cancer related medical services (hospitalizations, emergency department visits, office visits) and treatment (surgery, radiation, and pharmacotherapy) utilization among women recipients enrolled in a state Medicaid FFS program. • Objective 3: To determine the trends in breast cancer-related medical services and treatment costs among women recipients enrolled in a state Medicaid FFS program. • Objective 1: To determine the proportion of women ≥40 years of age in WV reporting not having a mammography screening in the past two years. • Objective 2: To determine the factors associated with women ≥40 years of age in WV reporting not having a mammography screening in the past two years. Funding support provided by: AHRQ P20 HS 01593 BACKGROUND RESULTS Breast cancer is the most frequently diagnosed non-skin malignancy and the second leading cause of cancer-related mortality among women in the United States (US). The incidence rates of breast cancer in the US decreased by 3.5%/year between 2001-2004, a trend partly attributed to decrease in screening. The total economic burden of breast cancer in the US is estimated to be ~$32-39 billion. Five-year survival rates and associated treatment costs vary by stage at diagnosis. Mammography screening is considered to be the gold standard for identifying early stage breast cancer, and recommended every year for women ≥40 years by the American Cancer Society (ACS). Breast cancer is also the most common cancer among women in West Virginia (WV). In 2005, the age-adjusted incidence rate (/100,000) was 114.5 for invasive and 25.1 for in-situ breast cancer in WV. Less than 1/5th of incident breast cancer cases in WV are diagnosed in-situ. SPECIFIC AIM 1 • In 2006 BRFSS, 25.5% of women ≥40 years of age in WV reported not having a mammogram in the past two years, as compared to 23.4% in the entire US (Table 1). • Among women respondents in WV, the proportion of respondents who had not had a mammogram in the past two years decreased significantly until the age of 64 years, and then reversed trend for those who were 65 years of age and above (p<0.001). • As education and income level increased, respectively, the proportion of women who had not had a mammogram in the past two years decreased significantly (p<0.001). • Healthcare access factors were found to be significantly (p<0.001) associated with women respondents reporting whether they had a mammogram in the past two years or not (Figure 1). • Factors including age, income, health insurance, availability of personal doctor, time since last routine checkup, and inability to see a healthcare provider because of cost were found to significantly predict whether women respondents ≥40 years of age in WV had a mammogram in the past two years or not (Table 2). SPECIFIC AIM 2 • Figure 2 shows the trends (2000-2005) in the prevalence of breast cancer among women recipients (21-64 years) enrolled in a state Medicaid FFS program. • Prevalence rate of breast cancer among women recipients in Medicaid increased from 11.3/1,000 in 2000 to 19.0/1,000 in 2005. • Prevalence rates were higher among women in the age group 60-64 years and those residing in rural counties as compared to women in the age group 21-59 years and residing in metro and non-metro urban counties, respectively. • Office visits accounted for a majority (>97%) of breast cancer-related medical services use among women recipients with a primary diagnosis of breast cancer in the state Medicaid (Figure 3). • The amount paid by the state Medicaid for breast cancer-related medical services and treatment use increased from ~$4.1 million in 2003 to $5.2 million in 2005 (Table 4). • In each of the three years (2003-2005), office visits accounted for >77% of the total costs incurred by the state Medicaid program. SPECIFIC AIM 1 - METHODOLOGY • Retrospective analysis of 2006 Centers for Disease Control and Prevention (CDC) Behavioral Risk Factor and Surveillance System (BRFSS) was conducted for specific aim 1. • The BRFSS is a state-based surveillance system that tracks information related to health behaviors and risk factors on a yearly basis. • The 2006 BRFSS data related to women ≥40 years of age in WV who reported as to whether they had a mammogram in the past two years or not were included for analysis and constituted the sample of interest for this aim. • Given the complex sampling design of BRFSS, analyses for this aim were conducted using SAS 9.1®. • Weighted proportions and 95% confidence intervals (CIs) were generated using PROC SURVEYFREQ. • Chi-square test was used to determine significant associations among categorical variables. • Logistic regression analysis (using PROC SURVEYLOGISTIC) was conducted to determine the factors associated with women in WV reporting not having a mammogram in the previous two years. SPECIFIC AIM 2 - METHODOLOGY Retrospective analysis of astate Medicaid FFS administrative claims dataset from January 1, 2000 to December 31, 2005 was conducted for specific aims 2 and 3. Objective 1 Objectives 2 and 3 Number of women (21-64 years) recipients with primary diagnosis of breast cancer (ICD-9-CM) in each year (2000-2005) Total number of women (21-64 years) enrolled in the Medicaid fee-for-service program in each year (2000-2005) Prevalence Rate (2000-2005) = SPECIFIC AIMS Specific Aim 1: To determine the factors associated with women reporting not having a mammography screening in WV. Specific Aim 2: To determine the trends in breast cancer prevalence and breast cancer-related healthcare utilization and costs among women recipients enrolled in a state Medicaid fee-for-service (FFS) program. Women recipients enrolled in a Medicaid fee-for-service program with a primary diagnosis of breast cancer (ICD-9-CM codes) in each year (2003-2005) Hospitalizations, Emergency Room, and Office Visits (Medical claims file) Treatment – Surgery and Radiation Therapy (Medical claims file); Chemotherapy and Hormone Therapy (Medical claims file and Prescription claims file) Figure 2: Trends in breast cancer prevalence rates (/1,000) among women recipients enrolled in a state Medicaid FFS program (2000-2005) Figure 1: Women ≥40 years in WV reporting not having a mammography screening in the past two years by healthcare access factors, BRFSS (2006) Table 1: Proportion of women ≥40 years in WV reporting not having a mammography screening in the past two years, BRFSS (2006) Table 2: Factors associated with women ≥40 years in WV reporting not having a mammography screening in the past two years, BRFSS (2006) A) Overall prevalence rate B) Prevalence rates by age category B) Personal doctor A) Health insurance CONCLUSIONS • Higher proportion of women ≥40 years of age in WV reported not having a mammogram in the past two years in comparison to the entire country. • Increasing prevalence of breast cancer among fee-for-service women recipients in the state Medicaid program is accompanied by increasing healthcare costs, a large majority of which is attributable to office services use. LIMITATIONS • For aim 1, causal inferences cannot be made between variables studied because of the cross-sectional nature of BRFSS survey. • As per aim 2, encounter data for recipients enrolled in Medicaid managed care plans were not available for this study. Therefore, the study results are not generalizable to the overall state Medicaid population. D) Prevalence rates by race C) Prevalence rates by location ***p<0.001 Table 4: Trends in breast cancer-related medical services and treatment costs among women recipients enrolled in a state Medicaid FFS program (2003-2005) C) Last routine checkup D) Unable to see doctor in the past 12 months because of cost Figure 3: Trends in breast cancer-related medical services use among women recipients enrolled in a state Medicaid FFS program (2003-2005) ***p<0.001 Table 3: Trends in breast cancer-related treatment use among women recipients enrolled in a state Medicaid FFS program (2003-2005) ***p<0.001; **p<0.01; *p<0.05





















