
BACKGROUND
Routine Use of Intraoperative Ultrasound Guidance during Intracavitary Brachytherapy Applicator Placement in Cervical Cancer: the University of Alabama at Birmingham (UAB) Experience Philip E. Schaner*, Jimmy J. Caudell* † , Jennifer F. DeLos Santos*, Sharon Spencer*, Sui Shen*, Robert Y. Kim*

BACKGROUND
E N D
Presentation Transcript
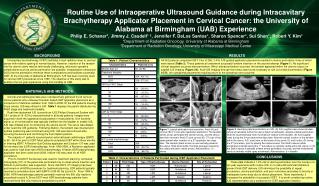
Routine Use of Intraoperative Ultrasound Guidance during Intracavitary Brachytherapy Applicator Placement in Cervical Cancer: the University of Alabama at Birmingham (UAB) Experience Philip E. Schaner*,Jimmy J. Caudell* †, Jennifer F. DeLos Santos*, Sharon Spencer*, Sui Shen*, Robert Y. Kim* *Department of Radiation Oncology, University of Alabama at Birmingham †Department of Radiation Oncology, University of Mississippi Medical Center BACKGROUND RESULTS • All 243 patients completed ICBT. Five of 356 (1.4%) IUS-guided applicator placements resulted in uterine perforation, three of which were lateral (Table 2). These patients all underwent successful tandem insertion on the second attempt (Figure 1). No significant clinical sequelae occurred after perforation. When lateral perforation occurred, the tandem appeared within the uterine corpus on sagittal IUS imaging (Figure 2A). Axial IUS imaging through the fundus was found necessary to rule out a lateral perforation (Figure2C-D).No suboptimal placements requiring return to the operating room occurred. Intracavitary brachytherapy (ICBT) facilitates a high radiation dose to cervical cancer with relative sparing of normal tissues.However, insertion of the tandem into the uterine cavity may be technically challenging, and acute operative complications such as uterine perforation are possible. Intraoperative ultrasound (IUS) has the potential to minimize these complications and facilitate successful ICBT. At the University of Alabama at Birmingham, IUS has been routinely used for cervical ICBT procedures since 1999. The objective of this study was to examine the ten year experience using this modality at UAB. MATERIALS AND METHODS Clinical and radiological data were retrospectively gathered for all cervical cancer patients who underwent tandem-based ICBT applicator placement as a component of definitive radiation from 1999 to 2008. Of the 259 patients meeting those criteria, IUS was utilized in 243. Table 1 displays the patient distribution by FIGO stage and treatment modality. Real-time abdominal IUS (currently an iU22 Philips Ultrasound System with C5-1 probe at 19 -22 Hz) was performed in all study patients. Images were acquired in both the sagittal and axial planes in most patients. One hundred eighty cc of normal saline was typically instilled into the bladder to enable IUS. IUS was initiated prior to introducing the uterine sound. The cervix was dilated under real-time IUS guidance. Following dilation, the tandem was inserted and optimal positioning was confirmed using IUS. IUS was discontinued after securing the device and confirming the final implant position. The majority of patients received pelvic external beam radiotherapy (EBRT) to 45 - 50.4 Gy prior to ICBT. Most patients completed ICBT within three months of finishing EBRT. A Fletcher-Suit-Delclos applicator with Cesium-137 was used for low dose rate (LDR) brachytherapy. From 1999-2006, a Nucletron applicator was used for high dose rate (HDR) brachytherapy. A Varian HDR brachytherapy applicator has been used since 2006. Iridium-192 was used for all HDR procedures. Prior to mid-2007 fluoroscopy was used for treatment planning; computed tomography (CT) of the pelvis was performed only in cases where insertion was difficult or perforation was suspected. Since mid-2007, CT imaging has been performed on all HDR procedures for treatment planning. LDR patients typically received a cumulative dose (with EBRT) of 80-90 Gy to point A. From 1999 to 2006, HDR brachytherapy patients generally received five 600 cGy fractions prescribed to point A. Since 2007 most HDR brachytherapy patients have received three 800 cGy fractions prescribed to point A. Figure 1: Lateral perforation and resolution. Axial (A) and coronal (B) CT scan after applicator placement. The tandem (white arrow) perforated the uterine serosa, and the device was then removed. Axial (C) and coronal (D) CT scan of the same patient after insertion of a 2nd applicator two days later. The tandem (black arrow) is now centrally placed in the uterus. Note blood within the false passage caused by the initial perforation (white arrow). Abbreviations: U = uterus. Figure 2: Identifying lateral perforation on IUS. (A) IUS (sagittal view) shows tandem (white arrowheads) within the uterus (black arrowheads), despite a lateral perforation. Note the asymmetrically thick myometrium relative to the tandem. (B) IUS (sagittal view) during the 2nd procedure two days later. Note the central location of the tandem within the uterus. IUS, axial view, at the levels of the cervix (C) and fundus (D) during the 2nd procedure, prior to placing the uterine sound. The Smit’s sleeve (white arrowhead) inserted during the 1st procedure is centrally visible within the uterus. In (D) the Smit’s sleeve is laterally evident where perforation occurred, and the endometrial cavity is centrally visible (grey arrowhead). Abbreviations: b = bladder. CONCLUSIONS These data indicate a 1.4% risk of uterine perforation over the course of a ten year experience with routine IUS; in no case did technical limitations prevent final ICBT delivery. IUS minimizes the possibility of repeat procedures, uterine perforation, and poor outcomes secondary to toxicity or inadequate tumor dose due to device placement. More importantly, it increases the probability of successful ICBT. It is worth considering routine IUS implementation as a component of ICBT applicator insertion.





















