Sodium, Potassium & Calcium
Sodium, Potassium & Calcium. Lab 9. Introduction. By definition, electrolytes are ions capable of carrying an electric charge. Essential component in numerous processes in the human body Volume and osmotic pressure Myocardial rhythm and contraction Cofactors in enzyme activation

Sodium, Potassium & Calcium
E N D
Presentation Transcript
Introduction • By definition, electrolytes are ions capable of carrying an electric charge. • Essential component in numerous processes in the human body • Volume and osmotic pressure • Myocardial rhythm and contraction • Cofactors in enzyme activation • Regulation of ATPase ion pump
Sodium • Sodium is the major cation of extracellular fluid. • It plays a central role in the maintenance of the normal distribution of water and the osmotic pressure in the various fluid compartments. • The main source of body sodium is sodium chloride contained in ingested foods. • Only about one-third of the total body’s sodium is contained in the skeleton since most of it is contained in the extracellular body fluids
Clinical Significance • Hyponatremia • Depletional • Renal or non-renal loss • Dilutional • Syndrome of inappropriate ADH • Generalised edema (Chronic heart failure) • Artifactual • Analytical error (hyperlipidemia, hyperproteinemia)
Clinical Significance • Hypernatremia • Water loss • GI loss, sweat loss, and diabetes insipidus • Sodium gain • Ingestion • Hyperaldosteronism • Acute renal failure • Changes in levels can cause symptoms of central nervous system origin and changes in thought processes and in the level of consciousness. • They presumably relate to changes in volume of the cells of the central nervous system (shrinkage with hypernatremia and swelling with hyponatremia), particularly if the condition has developed rapidly
Specimen Collection & Storage • Freshly drawn serum is the specimen of choice • Plasma from non-sodium containing anticoagulants (e.g., lithium, calcium, magnesium or heparin) is an acceptable alternative. • Sodium is stable for: • at least 24 hours at room temperature • and 2 weeks when refrigerated
Assay Principle • Sodium is precipitated as the triple salt, sodium magnesium uranyl acetate, • The excess uranium then being reacted with ferrocyanide, producing a chromophore • The absorbance varies inversely as the concentration of sodium in the test specimen.
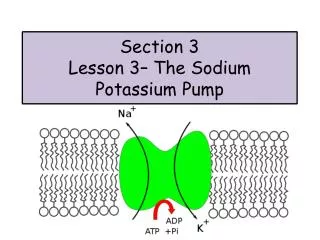
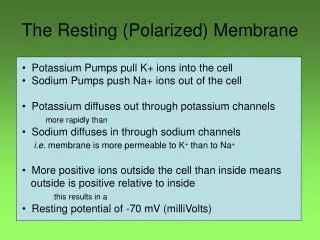
Potassium • Potassium is the principle cation of the intracellular fluid. • 20 X greater concentration in the cell vs. outside. • It is also an important constituent of the extracellular fluid due to its influence on muscle activity. • 2% of the bodies potassium circulates within the plasma. • Functions of Potassium include: • Regulates neuromuscular excitability • Hydrogen ion concentration • Intracellular fluid volume
Hypokalemia • Increased cellular uptake • Excess Insulin • Alkalosis • Renal loss • Hyperaldostronism • GI loss • Vomitting • Diarrhea
Hyperkalemia • Increased intake • Increased cell lysis • Altered cellular uptake • Acidosis • Insulin insufficiency • Impaired renal excretion
Specimen Collection & Storage • Serum is recommended. • Plasma from anticoagulants not containing potassium is also suitable. • Specimens for potassium analysis should be free from hemolysis • Blood specimens should also be separated from the red cells shortly after collection to prevent any leakage of potassium from the intracellular into the extracellular fluid. • Potassium in serum is stable for at least 2 weeks at 2 - 8°C.
Assay Principle • The amount of potassium is determined by using sodium tetraphenylboron in a specifically prepared mixture • This will produce a colloidal suspension • The turbidity of which is proportional to potassium concentration
Calcium • Calcium is the most abundant mineral in the human body, most of which (99%) is present in the bone. • The remaining calcium is found in plasma • Calcium plays a very important role in bone mineralization, and it is also vital for basic physiologic processes such as blood coagulation, neuromuscular conduction.
Calcium (Ca2+) is present in the blood in two forms: • Approximately 45% is present in a free state, • and the other 55% is bound to plasma protein, primarily to albumin. • Ionized calcium is the metabolically active form of calcium. • Level is affected by the albumin level, blood pH, and others • Decreased by factors that bind calcium (citrate from transfused blood or free fatty acids from total parenteral nutrition [TPN]).
Total calcium is a measurement of both bound and free calcium. • This provides information regarding parathyroid gland function and the metabolism of calcium. • A major cause of hypercalcemia is neoplasia; increases are observed in primary bone disease such as multiple myeloma and in bone metastases.
Since much of the circulating calcium is bound to albumin, calcium levels in the blood must be interpreted in relation to serum albumin levels. • As serum albumin decreases 1 g/dl, the total serum calcium decreases approximately 0.8 mg/dl due to the decrease in the bound calcium; • the amount of free calcium would not change.
Hypocalcemia • Hypoparathyroidism, Vitamin D deficiency • Renal disease • Hypoalbuminemia (total calcium only, ionized not affected) • Hypercalcemia • Hyperparathyroidism • Malignancy (many tumors produce PTH-related peptide (PTH-rP), which binds to normal PTH receptors • hyperthyroidism can sometimes cause hyperparathyroidism because of the proximity
Specimen • Serum or heparinized plasma or 24 Hrs urine • Separation from cells as rapidly as possible to avoid the uptake of calcium by erythrocytes. • Venous stasis (prolonged tourniquet application) and forearm exercise may increase ionized calcium due to a decrease in pH caused by localized production of lactic acid. • Exposing the sample to air will cause an increase in pH due to the loss of CO2 which will decrease ionized calcium. • Storage and stability:
Methods of Determination • Ionized Calcium – (Ca2+) – ion-selective electrodes • Total Calcium • Colorimetric – Calcium in alkaline solution reacts with o-cresolphthalein and Complexone to form a purple complex which is proportional to the calcium concentration.
Coloremetric end-point reaction • Photometric test using cresolphtalein complexone (CPC). • Cresolphthalein complexone reacts with calcium ions in alkaline medium forming a red-violet color: • Interference by magnesium is eliminated by addition of 8-hydroxyquinoline. • The absorbance at 575 nm is directly proportional to the calcium concentration in the sample.