Download
1 / 20
1.02k likes | 3.86k Views
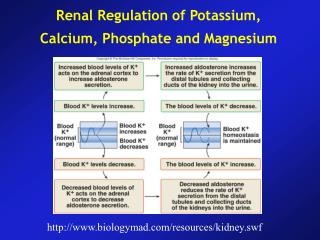
Renal Regulation of Potassium, Calcium, Phosphate and Magnesium. http://www.biologymad.com/resources/kidney.swf. Regulation of Potassium (K) Excretion. Extracellular K concentration is about 4.2 mEq/L Daily K intake is between 50 to 200 mEq/L Hyperkalemia Hypokalemia.

E N D
Renal Regulation of Potassium, Calcium, Phosphate and Magnesium http://www.biologymad.com/resources/kidney.swf
Regulation of Potassium (K) Excretion • Extracellular K concentration is about 4.2 mEq/L • Daily K intake is between 50 to 200 mEq/L • Hyperkalemia • Hypokalemia
Regulation of Internal K Distribution • Insulin stimulates K uptake into cells • Aldosterone increases K uptake into cells • Beta-adrenergic stimulation increases cellular uptake of potassium • Acid-base abnormalities can cause changes in K distribution • Metabolic acidosis increases and alkalosis decreases extracellular K levels • Cell lysis causes increased extracellular K concentration • Strenuous exercise can cause hyperkalemia by releasing K from skeletal muscle • Increased extracellular fluid osmolarity causes redistribution of K from the cells to extracellular fluid
Renal Potassium Excretion • K excretion is determined by three processes: • Rate of K filtration • Rate of K reabsorption and • Rate of K secretion by the tubules
Renal Potassium Excretion • The most important sites for regulating K excretion are the principal cells of the late distal tubules and cortical collecting tubules
Renal Potassium Excretion • Increased extracellular K concentration • Increased aldosterone and • Increased tubular flow rate stimulate secretion of K by the principal cells
Lack of Aldosterone Feedback Mechanism Impairs Control of K Concentration • In the absence of aldosterone secretion (as in Addison’s disease) extracellular K levels are impaired (increase) • Conversely, with excess aldosterone secretion (primary aldosteronism) K loss by the kidneys is greatly increased (hypokalemia)
Control of Renal Calcium Excretion • Extracellular Ca concentration is regulated tightly (2.4 mEq/L) • Hypercalcemia • Hypocalcemia • Changes in plasma H concetration can influence the degree of Ca binding to plasma proteins • With acidosis, less Ca is bound to proteins, in alkalosis great amount of Ca is bound to plasma proteins • Patients with alkalosis are more suceptible to hypocalcemic tetany
Control of Renal Calcium Excretion • 99 % of the total Ca is stored in the bone • Only 1 % is in the extracellular fluid • And 0.1% in the intracellular fluid • Daily dietary intake is about 1000 mg • About 900 mg Ca is lost in feces daily • One of the most important regulators of bone uptake and release of Ca is PTH • PTH stimulates bone resorption • Stimulates Vit D which increases GI absorption of Ca • Directly increases renal tubular reabsorption of Ca
Control of Calcium Excretion by the Kidneys • Renal Ca excretion = Ca filtered – Ca reabsorbed • Normally, 99 % of the Ca filtered is reabsorbed • 65% of it is absorbed in the PCT • 25% in the ascending Henle • And 5-10% in the distal and collecting tubules • Its reabsorption pattern is similar to that of Na
Control of Calcium Excretion by the Kidneys • Primary controller of renal tubular reabsorption is PTH • Another factor is the plasma concentration of phosphate • Increased phosphate stimulates (??) PTH which increases reabsorption of Ca (thus reduces excretion) • Ca reabsorption is also stimulated by metabolic acidosis and inhibited by metabolic alkalosis
Regulation of Renal Phosphate Excretion • The renal tubules have a normal transport maximum for reabsorbing phosphate of about 0.1mM/min • When less than this amount is present in the glomerular filtrate, all phosphate is reabsorbed … • PTH plays a significant role in phosphate excretion: 1) PTH promotes bone resorption (Ca and phosphate) 2) It decreases transport maximum of phosphate • Thus whenever PTH is increased, phosphate reabsorption is decreased and excretion is increased
Role of PTH • Stimulates renal reabsorption of calcium • Inhibits renal reabsorption of phosphate • Stimulates bone resorption • Inhibits bone formation and mineralization • Stimulates synthesis of calcitriol ↑ serum calcium ↓ serum phosphate Net effect of PTH
Control of Renal Magnesium Excretion • Most of the Mg is stored in the bones • Most of the other half is found in the cells • Only about 1 % is located in the extracellular fluid • Total plasma Mg level is about 1.8 mEq/L • Most of it is bound to plasma proteins • Free ionized Mg concentration is only about 0.8 mEq/L • Daily intake of Mg is about 250 mg • Only about half of it is absorbed in the GI tract • Thus the kidneys must excrete this absorbed amount
Control of Renal Magnesium Excretion • Regulation of Mg is mainly achieved by tubular reabsorption • Only about 25 % of filtered Mg is reabsorbed in the PCT • Most of it (65%) is reabsorbed in the ascending Henle • The remaining 5-10% is reabsorbed in the distal and proxymal collecting tubules