Download
1 / 74
740 likes | 761 Views
Learn about palliative care, which affirms life and provides relief from pain and symptoms. Discover the WHO's analgesia ladder and the importance of a balanced diet and physical activity for maintaining overall well-being.

E N D
WHO defines palliative care as an approach that : Affirms life and regards death as a normal process. Does not hasten or postpone death. Provides relief from pain and other symptoms. Offers a support system to help patients live as actively as possible right up to their death. Integrates psychological and spiritual care. Provides a wider support to help the family cope during the patient’s illness and their own bereavement after death.
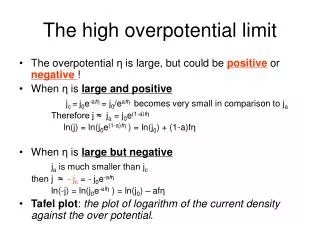
Pain control is central to palliative care, and presents challenges in itself. The analgesia ladder, as developed by WHO, includes three steps:Step 1 : Aspirin or paracetamol.Step 2 : Codeine or dihydrocodeine, with or without non-steroidal or anti-inflammatory drugs such as ibuprofen or indomethacin.Step 3 : Morphine, with or without co-analgesia, and with or without steroid anti-inflammatory drugs.Other strong opioid analgesics include pethidin and fentanyl.
Eat five or more servings of a variety of vegetables and fruits each day. * Include vegetables and fruits at every meal and for snacks. * Eat a variety of vegetables and fruits. * Limit French fries, snack chips, and other fried vegetable products. * Choose 100% juice if you drink fruit or vegetable juices.
Choose whole grains in preference to processed (refined) grains and sugars. * Choose whole grain rice, bread, pasta, and cereals. * Limit consumption of refined carbohydrates, including pastries, sweetened cereals, soft drinks, and sugars.
Limit consumption of red meats, especially those high in fat and processed. * Choose fish, poultry, or beans as an alternative to beef, pork, and lamb. * When you eat meat, select lean cuts and smaller portions. * Prepare meat by baking, broiling, or poaching, rather than by frying or charbroiling.
Choose foods that help maintain a healthful weight • When you eat away from home, choose food low in fat, calories, and sugar • and avoid large portions. • Eat smaller portions of high-calorie foods. Be aware that
Examples of Moderate and Vigorous Physical Activities Moderate Activities Vigorous Activities Exercise and Leisure Walking, dancing, Leisurely bicycling, ice-skating or roller- skating, horseback riding, canoeing, yoga Jogging or running, fast bicycling, circuit weight training, aerobic dance, martial arts, jump rope, swimming Volleyball, golfing, softball, baseball Soccer, field hockey or ice hockey, lacrosse, singles
Moderate Activities Vigorous Activities Sports Badminton, doubles tennis, downhill skiing tennis, racquetball, basketball, cross country skiing Home Activities Mowing the lawn, general lawn and garden maintenance Digging, carrying and hauling, masonry, carpentry Heavy manual labor (forestry, construction, fire fighting) Walking and lifting as part of the job (custodial work, farming, auto or machine repair) Occupational Activity
Helpful Ways to Be More Active • Use stairs rather than an elevator. • If you can, walk or bike to your destination. • Exercise at lunch with your workmates, family, or friends. • Take a 10-minute exercise break at work to stretch or take a quick • walk. • Walk to visit co-workers instead of sending an email. • Go dancing with your spouse or friends. • Plan active vacations rather than only driving trips. • Wear a pedometer every day and watch your daily steps increase. • Join a sports team. • Use a stationary bicycle while watching TV. • Plan your exercise routine to gradually increase the days per week • and minutes per session.
Maintain a healthful weight throughout life. Balance caloric intake with physical activity. Lose weight if currently overweight or obese. Being overweight or obese is associated with an increased risk of developing several types of cancer: • Breast (among postmenopausal women) • Colon • Endometrium • Esophagus • Gallbladder • Pancreas • Kidney
If you drink alcoholic beverages, limit consumption. People who drink alcohol should limit their intake to no more than 2 drinks per day for men and 1 drink a day for women. The recommended limit is lower for women because of their smaller body size and slower metabolism of alcohol. A drink is defined as 12 ounces of beer, 5 ounces of wine, or 1.5 ounces of 80 proof distilled spirits.
Alcohol is an established cause of cancers of the: • Mouth • Pharynx (throat) • Larynx (voice box) • Esophagus • Liver • Breast Alcohol may also increase the risk of colon cancer.
Diet and Physical Activity Factors That Affect Risks for the Most Common Cancers Although the nutrition and activity guidelines are intended to reduce overall cancer risk, certain dietary and physical activity habits affect the risk for developing specific types of cancer. This section summarizes the relation of diet and physical activity factors to the common cancers in the United States.
Bladder Cancer The major risk factors for bladder cancer are tobacco smoking and exposure to certain industrial chemicals. However, drinking more fluids and eating more vegetables may lower the risk of bladder cancer. Brain Cancer There are no know nutritional risk factors for brain cancer.
Breast Cancer The risk of breast cancer is increased by several factors that cannot be easily changed: • Having your first period before age 12 • Not having children or having your first birth after age 30 • Late age at menopause • Family history of breast cancer Other factors that increase risk, however, can be changed by : • Limiting the use of hormones (hormone replacement therapy) • Reducing alcohol consumption • Breastfeeding • Avoiding obesity • Being physically active
The best advice to reduce the risk of breast cancer is to: • Engage in vigorous physical activity at least 4 hours a week • Avoid or limit your intake of alcohol to no more than one drink per • day • Reduce lifetime weight gain through the combination of limiting • your calories and exercising regularly
Colorectal Cancer The best advice to reduce the risk of colon cancer is to: • Increase your physical activity • Eat more vegetables and fruit • Limit intake of red meats • Avoid obesity • Avoid excess alcohol
Endometrial Cancer Studies of endometrial cancer (cancer of the lining of the uterus) show that obesity and use of hormonal replacement therapy after menopause increase risk. The link to weight is thought to result from the increase in estrogen levels that occurs among postmenopausal women who are overweight. The best advice to reduce the risk of endometrial cancer is to maintain a healthful weight through diet and regular physical activity.
Kidney Cancer Kidney cancer risk is increased among those who are overweight. The reason for this is unknown. The best nutritional advice to lower risk for kidney cancer is to avoid becoming overweight. Leukemias and Lymphomas There are no Known nutritional risk factors for leukemias or lymphomas.
Lung Cancer More than 85% of lung cancers result from tobacco smoking. Many studies have shown that the risk of lung cancer is lower among both smokers and nonsmokers who consume at least five servings of vegetables and fruits a day. Although healthful eating may reduce the risk of lung cancer, the risks from tobacco smoking, chewing tobacco, and snuff remain substantial. Using high doses of beta-carotene and/or vitamin A has increased (not decreased) lung cancer risk among smokers (see beta-carotene under Common Questions About Diet and Cancer). The best advice to reduce the risk of lung cancer is to avoid tobacco use or exposure and to eat at least five servings of vegetables and fruits every day.
Oral and Esophageal Cancers The best advice to reduce the risk of oral and esophageal cancers is to: • Avoid all forms of tobacco • Restrict alcohol consumption • Avoid obesity • Eat at least five servings of vegetables and fruits each day
Pancreatic Cancer The best advice to reduce the risk of pancreatic cancer is to: • Avoid tobacco use • Maintain a healthful weight • Remain physically active • Eat five or more servings of vegetables and fruits each day
Prostate Cancer For now, The best advice to reduce the risk of prostate cancer is to: • Limit intake of animal products, especially red meat and high-fat • dairy products • Eat five or more servings of vegetables and fruits each day
Stomach Cancer The rates of stomach cancer are decreasing as a result of the reduced prevalence of chronic stomach infections by the bacterium Helicobacter pylori. Year-round consumption of fresh foods made possible by refrigeration and other improvements in food preservation methods also have likely helped to reduce the rates. At this time, the best advice to reduce the risk of stomach cancer is to eat at least five servings of vegetables and fruits daily.
Complementaryrefers to supportive methods that are used to Complement, or add to, mainstream treatments. Examples might include meditation to reduce stress, peppermint tea for nausea, and acupuncture for chronic back pain. Complementary methods are not given to cure disease, rather they may help control symptoms and improve well-being. Some of the methods, such as massage therapy, yoga, and meditation, that are categorized as complementary have actually been referred to as supportive care in the past.
Alternative refers treatments that are promoted as cancer cures. Theyare unproven because they have not been scientifically tested, or weretested and found to be ineffective. If used instead of evidence-basedtreatment, the patient may suffer, either from lack of helpful treatment orbecause the alternative treatment is actually harmful.
Some Helpful Complementary Approaches • aromatherapy • art therapy • biofeedback • massage therapy • meditation • music therapy • prayer, spiritual practices • t’ai chi • yoga
Questions to Ask About Alternative and complementary Therapies • What claims are made for the treatment: to cure the cancer or to enable the • evidence-based treatment to work better? To relieve symptoms or side • effects? • What are the credentials of those supporting the treatment? Are they • recognized experts in cancer treatment? Have they published their findings • in trustworthy journals? • How is the method promoted? Is it promoted only in the mass media (books, • magazines, TV and radio talk shows) rather than in scientific journals? • What are the costs of the therapy? • Is the method widely available for use within the health-care community, • or is it controlled with access to its use limited? • If used in place of standard therapies or clinical trials, will the
Ensuing delay affect any chances for cure or advance the cancer stage? Signs of Treatments to avoid • Is the treatment based on an unproven theory? • Does the treatment promise a cure for all cancers? • Are you told not to use conventional medical treatment? • Is the treatment or drug a “secret” that only certain providers can give? • Does the treatment require you to travel to another country? • Do the promoters attack the medical/scientific establishment?
Breast • Yearly mammograms are recommended starting at age 40.The age at which • screening should be stopped should be individualized by considering the • potential risks and benefits of screening in the context of overall health status • and longevity. • Clinical breast exam should be part of a periodic health exam, about every • three years for women in their 20s and 30s,and every year for women 40 • and older. • Women should know how their breasts normally feel and report any breast • change promptly to their health care providers. Breast self-exam is an option • for women starting in their 20s. • Women at increased risk (e.g.,family history, genetic tendency, past breast • cancer)should talk with their doctors about the benefits and limitations of • starting mammography screening earlier, having additional tests (I.e.,breast • ultrasound and MRI), or having more frequent exams.
Colon & rectum • Beginning at age 50, men and women should follow one of the examination • schedules below: • A fecal occult blood test (FOBT) or fecal immunochemical test (FIT) every • year • A flexible sigmoidoscopy (FSIG) every five years • Annual FOBT or FIT and flexible sigmoidoscopy every five years* • A double-contrast barium enema every five years • A colonoscopy every 10 years • *Combined testing is preferred over either annual FOBT or FIT, or FSIG • every five years,alone.People who are at moderate or high risk for colorectal • cancer should talk with a doctor about a different testing schedule.
Prostate The PSA test and the digital rectal examination should be offered annually, beginning at age 50, to men who have a life expectancy of at least 10 years. Men at high risk (African American men and men with a strong family history of one or more first-degree relatives diagnosed with prostate cancer at an early age)should begin testing at age 45. For both men at average risk and high risk, information should be provided about what is known and what is uncertain about the benefits and limitations of early detection and treatment of prostate cancer so that they can make an informed decision about testing.
Uterus Cervix : Screening should begin approximately three years after a woman begins having vaginal intercourse, but no later than 21 years of age. Screening should be done every year with regular Pap tests or every two years using liquid-based tests. At or after age 30, women who have had three normal test results in a row may get screened every two to three years.Alternatively,cervical cancer screening with HPV DNA testing and conventional or liquid-based cytology could be performed every three years. However, doctors may usggest a woman get screened more often if she has certain risk factors, such as HIV infection or a weak immune system.Women 70 years and older who have had three or more consecutive normal Pap tests in the last 10 years may choose to stop cervical cancer screening. Screening after total hysterectomy (with removal of the cervix) is not necessary unless the surgery was done as a treatment for cervical cancer.
Endometrium: The American Cancer Society recommends that at the time of menopause all women should be informed about the risks and symptoms of endometrial cancer, and strongly encouraged to report any unexpected bleeding or spotting to their physicians. Annual screening for endometrial cancer with endometrial biopsy beginning at age 35 should be offered to women with or at risk for hereditary nonpolyposis colon cancer (HNPCC).
Moderate Physical Activity Examples* Washing and waxing a car for 45-60 minutes Washing windows or floors for 45-60 minutes Playing touch football for 30-45 minutes Playing volleyball for 45 minutes Playing touch football for 30-45 minutes Gardening for 30-45 minutes Wheeling self in wheelchair for 30-40 minutes Walking 1 3/4 miles in 35 minutes (20 minutes per mile) Basketball (shooting baskets) for 30 minutes Bicycling for 5 miles in 30 minutes Dancing fast (social) for 30 minutes Pushing a stroller 1 1/2 miles in 30 minutes Raking leaves for 30 minutes Walking 2 miles in 30 minutes (15 minutes per mile) Water aerobics for 30 minutes Swimming laps for 20 minutes Wheelchair basketball for 20 minutes Basketball (playing a game) for 15-20 minutes Bicycling 4 miles in 15 minutes Jumping rope for 15 minutes Running 1 1/2 miles in 15 minutes (10 minutes per mile) Shoveling snow for 15 minutes Stairwalking for 15 minutes Less Vigorous, More Time More Vigorous, Less Time *The amount of physical activity is influenced by its duration, intensity, and frequency.The same amount of activity can be obtained in longer sessions of moderately intense activities (such as brisk walking) as in shorter sessions of more strenuous activities (such as running). Adapted from: Chronic Disease Notes & Reports, a publication of the Centers for Disease Control and Prevention.111 • To achieve the American Cancer Society physical activity guidelines, adults may choose a variety of • activities. Some examples from the table above include: • Bicycle 5 miles in 30 minutes • Walk 2 miles in 30 minutes and run 11/2 miles in 15 minutes • Garden for 30 minutes • Play volleyball for 45 minutes
American Cancer Society Guidelines on Nutrition and Physical Activity for Cancer Prevention • Recommendations for individuals • 1. Eat a variety of healthful fools, with an emphasis on plant sources. • Eat five or more servings of a variety of vegetables and fruits each day. • Choose whole grains in preference to processed (refined) grains and sugars. • Limit consumption of red meats, especially high-fat and processed meats. • Choose foods that help maintain a healthful weight. • 2. Adopt a physically active lifestyle. • Adults should engage in at least moderate activity for 30 minutes or more on five or more days of • the week; 45 minutes or more of moderate to vigorous activity on five or more days per week may • further enhance reductions in the risk of breast and colon cancer. • Children and adolescents should engage in at least 60 minutes per day of moderate to vigorous • physical activity at least five days per week. • 3. Maintain a healthful weight throughout life. • Balance caloric intake with physical activity. • Lose weight if currently overweight or obese. • 4. If you drink alcoholic beverages, limit consumption. • Recommendation for Community Action • Public, private, and community organizations should work to create social and physical environments • that support the adoption and maintenance of healthy nutrition and physical activity behaviors. • Increase access to healthful foods in schools, worksites, and communities. • Provide safe, enjoyable, and accessible environments for physical activity in schools and for • transportation and recreation in communities.
WHODEFINITION OF PALLIATIVE CARE Palliative care is an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual. Palliative care:
provides relief from pain and other distressing symptoms; • affirms life and regards dying as a normal process; • intends neither to hasten or postpone death; • integrates the psychological and spiritual aspects of patient care; • offers a support system to help patients live as actively as possible until • death; • offers a support system to help the family cope during the patient’s illness • and in their own bereavement; • uses a team approach to address the needs of patients and their families, • including bereavement counselling, if indicated; • will enhance quality of life, and may also positively influence the course of • illness; • is applicable early in the course of illness, in conjunction with other thera- • pies that are intended to prolong life, such as chemotherapy or radiation • therapy, and includes those investigations needed to better understand • and manage distressing clinical complications.
ประเด็นปัญหาที่พบในผู้ป่วยระยะสุดท้ายประเด็นปัญหาที่พบในผู้ป่วยระยะสุดท้าย ปัญหาเศรษฐกิจ 1.1 ช่วยเหลือด้านค่ารักษาพยาบาล ร้อยละ 30.0 1.2 ช่วยเหลือสนับสนุนให้ได้รับสิทธิพึงมีพึงได้ด้านการรักษาพยาบาล ร้อยละ 58.3 1.3 ช่วยเหลือด้านค่าครองชีพ/เงินทุนประกอบอาชีพเพื่อช่วยเหลือครอบครัว 24 ราย/ปี 1.4 ช่วยเหลือด้านค่าพาหนะไป-กลับ 25 ราย/ปี 1.5 ช่วยเหลือด้านการจัดรถหรือใช้รถพยาบาล ไปส่งผู้ป่วยกลับบ้าน โรงพยาบาลใกล้บ้าน 20 ราย/ปี 1.6 จัดกิจกรรมฝึกอาชีพส่งเสริมอาชีพให้ครอบครัว 2 ครั้ง/เดือน 1.7 ช่วยเหลือโลงศพและผ้าขาวห่อศพ ในกรณีผู้ป่วยยากไร้ 12 ราย/ปี 1.8 ช่วยเหลือค่าใช้จ่ายเป็นกิจกรรมฌาปนกิจศพ ในผู้ป่วยยากไร้ 7 ราย/ปี 1.9 ช่วยเหลือจัดการฌาปนกิจศพ ให้แก่ผู้ป่วยไม่มีญาติ / ตามความต้องการของผู้ป่วย 4 ราย/ปี 1.10 ช่วยเหลืออุปกรณ์ทางการแพทย์ - รถเข็น / Walker 7 ราย/ปี - ให้ยืมเตียงและเบาะลมหมุนเวียนไปใช้จนกว่าผู้ป่วยเสียชีวิตและนำมาคืนเพื่อให้ ผู้ป่วยรายอื่นต่อไป 12 ราย/ปี - ให้ยืมเครื่องดูดเสมหะ / ถังออกซิเจน / เครื่องช่วยหายใจ 14 ราย/ปี
การช่วยเหลือทางจิตใจและสังคมการช่วยเหลือทางจิตใจและสังคม (Psychosocial Support) หลักการของการบริบาล (Principle of Care) 1. Concern หมายถึง ความผูกพัน ความห่วงใย 2. Clinical competence หมายถึง ความสามารถทางคลินิก 3. Comfort หมายถึง การปลอมโยน 4. Compassion หมายถึง ความกรุณา 5. Communication หมายถึง การสื่อสาร 6. Children หมายถึง เด็ก ๆ หรือลูกหลาน 7. Cohesion หมายถึง ความเชื่อมแน่น 8. Cheerfulness หมายถึง ความร่าเริง ความจริง 9. Consistency หมายถึง ความคงเส้นคงวา ขอเพิ่มสาม E สำหรับแพทย์ที่รับผิดชอบในการดูแลผู้ป่วยในระยะสุดท้าย คือ 1) Empathy หมายถึง ความร่วมรู้สึกหรือการมีอารมณ์ร่วมกัน 2) Encouragement หมายถึง การสนับสนุนเป็นลักษณะของการให้กำลังใจ 3) Equanimity หมายถึง อุเบกขา คือความมีใจเป็นกลาง
ประเด็นจริยธรรมของการดูแลด้านจิตวิญญาณประเด็นจริยธรรมของการดูแลด้านจิตวิญญาณ 1. การบอกข้อมูลและการบอกความจริง (veracity, truth telling) 2. การบรรเทาความเจ็บปวด 3. การตัดสินใจเลือกวิธีการรักษาในหออภิบาลผู้ป่วยหนัก 4. ลางสังหรณ์ใกล้ตาย (Symbolic expression of dying patient) 5. การตอบสนองทางด้านจิตวิญญาณเมื่อวาระสุดท้ายมาถึง
Breaking bad news หลัก 6 ขั้นตอนของ Robert Buckman 1. การเตรียมความพร้อม 2. ประเมินว่าผู้ป่วยรู้เรื่องของโรคมากน้อยแค่ไหน 3. ประเมินว่าผู้ป่วยต้องการรู้ข่าวสารมากน้อยเพียงใด 4. แลกเปลี่ยนข่าวสาร 5. ตอบสนองต่ออารมณ์ของผู้ป่วย 6. การวางแผนและติดตามการรักษา
Dying Patients Elizabeth Kubler Ross ได้รวบรวมข้อมูลจากประสบการณ์กับผู้ป่วยมะเร็งและ สรุปเป็นปฏิกิริยาการปรับตัวของผู้ป่วยเพื่อรับกับความตาย ดังนี้ 1. The stage of denial 2. The stage of anger 3. The stage of bargaining 4. The stage of depression 5. The stage of acceptance
Medical professionals involved in breast cancer diagnosis and treatment may include: • Gynecologist or OB/GYN, family practitioner, or other primary care physician • Radiologist • Oncologist (general, medical, radiation, surgical) • Oncology nurse specialist • Oncology social works • Surgeon • Radiation therapy oncologist • Radiation therapy technologist • Radiation therapy physicist • Pathologist • Reconstructive/plastic surgeon
Life Beyond Cancer • Post-Treatment Resource Program Our Post-Treatment Resource Program offers help to former cancer patients and their families. • Educational Support Groups Educational support groups led by Post-Treatment Resource Program staff. • Upcoming Programs Continually updated information about upcoming educational support groups. • Counseling, Wellness & Complementary Medicine Information about our support groups, seminars, workshops, and one-on-one counseling for cancer survivors. • Sexual Health Help with issues of sexual health related to cancer and its treatment.
Survivorship & Support • Follow-up Care • Management of Complications • Other Aspects of Survivorship
Outpatient Counseling • Individual, Family & Group Counseling • Alleviating Distress & Other Symptoms • Mindfulness-based Stress Reduction • Quitting Smoking & Improving Health Habits • Neuropsychological Testing • Art Therapy • AIDS Supportive Care Program • Research Studies • For Information about Counseling Center Services
Post-Treatment Resource Program • individual and family consultations • seminars and workshops • professionally led support groups • practical advice on insurance and employment issues
Educational Support Groups • Autologous Stem Cell Transplant: Transitions • Bladder Cancer: Challenges & Solutions • Esophagectomy: Finding a new balance • Grace & Grit: A Women’s Circle • Head, Neck, and Oral Cancers: Moving Forward • Living Well Programs • Lung Cancer: Breathing Easier • Men & Cancer: Maintaining Focus • Primary Brain Tumors: A Gathering for Patients and Families • Time and Again: Living On and Off Treatment • Young Adults: New Challenges/New Beginnings