Real-time control
Insulin. Brain. Plasma Insulin. Insulin losses (liver, kidneys). Blood Glucose. Effective insulin. Pancreas. Glucose. Insulin sensitivity. Liver. Other cells. Retrospective data. Real-time control. Virtual in-silico trials. Before: wide BG spread. After: tight BG spread.

Real-time control
E N D
Presentation Transcript
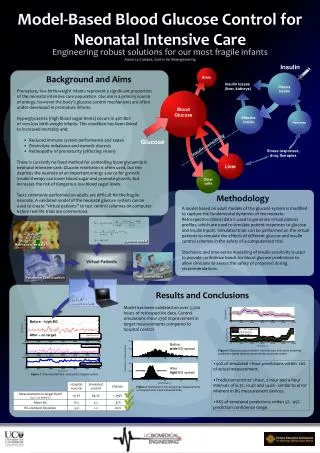
Insulin Brain Plasma Insulin Insulin losses (liver, kidneys) Blood Glucose Effective insulin Pancreas Glucose Insulin sensitivity Liver Other cells Retrospective data Real-time control Virtual in-silico trials Before: wide BG spread After: tight BG spread Model-Based Blood Glucose Control for Neonatal Intensive Care Engineering robust solutions for our most fragile infants Aaron Le Compte, Centre for Bioengineering Background and Aims • Premature, low-birth-weight infants represent a significant proportion of the neonatal intensive care population. Glucose is a primary source of energy, however the body’s glucose control mechanisms are often under-developed in premature infants. • Hyperglycaemia (high blood sugar levels) occurs in 40%-80% • of very low birth weight infants. This condition has been linked • to increased mortality and: • Reduced immune system performance and sepsis • Electrolyte imbalance and osmotic diuresis • Retinopathy of prematurity (affecting vision) • There is currently no fixed method for controlling hyperglycaemia in neonatal intensive care. Glucose restriction is often used, but this deprives the neonate of an important energy source for growth. Insulin therapy can lower blood sugar and promote growth, but increases the risk of dangerous low blood sugar levels. • Tests commonly performed on adults are difficult for the fragile neonate. A validated model of the neonatal glucose system can be used to create “virtual patients” to test control schemes on computer before real-life trials are commenced. Stress responses, drug therapies Methodology A model based on adult models of the glucose system is modified to capture the fundamental dynamics of the neonate. Retrospective clinical data is used to generate virtual patient profiles, which are used to simulate patient responses to glucose and insulin inputs. Simulated trials can be performed on the virtual patients to simulate the effects of different glucose and insulin control schemes in the safety of a computerised trial. Stochastic and time-series modelling of insulin sensitivity is used to provide confidence bands for blood glucose predictions to allow clinicians to assess the safety of proposed dosing recommendations. System model Parameter identification Results and Conclusions Model has been validated on over 3,500 hours of retrospective data. Control simulations show 239% improvement in target measurements compared to hospital control Before – high BG After – on target Figure 3: Blood glucose prediction intervals (top) and insulin sensitivity predictions bands (bottom) generated by stochastic model. • 90% of simulated 1-hour predictions within 20% of actual measurement. • Prediction error at 1-hour, 2-hour and 4-hour intervals of 6.3%, 10.4% and 14.6% - similar to error inherent in BG measurement devices. • 88% of simulated predictions within 5% - 95% prediction confidence range. Figure 1: Simulated BG trial compared to hospital control Figure 2: Distribution of blood glucose measurements on hospital control and simulated trials.