Download
1 / 30
340 likes | 417 Views
COMMUNITY HEALTH WORK IN SUB-SAHARAN AFRICA: The Kenyan experience

E N D
COMMUNITY HEALTH WORK IN SUB-SAHARAN AFRICA: The Kenyan experience The role of CHWs in sub-Saharan Africa has evolved over time and place in response to changing health care priorities, disease burdens, and shortages of human resources for health. CHW programmes play a crucial role in the support and delivery of services in sub-Saharan Africa and are critical in efforts to tackle the existing health worker crisis. However, they need support, supervision and financial and non-financial incentives if they are to carry out their work effectively. This session will look at how one such CHW programme in a South Kenyan district at the foot of Mt.Kilimanjaro informs the above issues. Presented by: Dr. Edwin Lutomia Mangala MSc. Public health-health promotion student Leeds Metropolitan University.
Objectives • To analyse, through a practical example, the role of CHWs in public health in Sub-Saharan Africa • To identify some of the key challenges that face CHW programs • To explore possible solutions to identified challenges
Scope • Background information • Social, political, economic • The healthcare system • The CHW program in Loitokitok district • Design and implementation • Early challenges and intervening measures • Successes and failures • Key issues arising
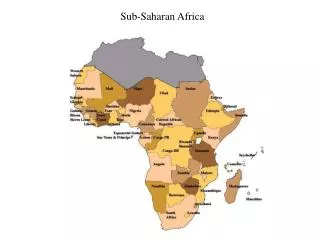
Background • Sub-Saharan Africa & Kenya
Country Profile • Geography • 580,367sq.km • Capital – Nairobi • Other cities – Mombasa, Kisumu • People • Population – 39m • Religion – Christian 82.6%, Muslim 11.2%, Traditional 5% • Languages • Official – English, Swahili • Others – 40 from Bantu (67%), Nilotic (30%) and cushitic (3%) • Government • President • Prime Minister • Economy • Largest in Eastern Africa • Services – 59.5% • Agriculture – 23.8% • Industry and commerce – 16.7% • Political • Multiparty state in 1992 • New constitution 2010 • Over 40 political parties
Kenya health care system • Ministry of Health • Ministry of Medical Services • Ministry of Public Health and Sanitation • Two broad divisions • Public (government owned) • Private
Kenya Healthcare system • Traditional pyramidal structure • Dispensaries and private clinics • Health centres • Sub-district hospitals and nursing homes • District hospitals and private hospitals • Provincial hospitals (8) • National hospitals (2)
Important Institutions • Medical practitioners and dentists board • Clinical officers council • Nursing council of Kenya • Kenya medical supplies agency (KEMSA) • Pharmacy and Poisons Board • National hospital insurance fund (NHIF) • Kenya Medical Research Institute (KEMRI)
Source: WHO (2009) • Budgetary allocation to health fell from 7% (2009/2010) to 6.5%; Target 15%
Some key health/Development Indicators Source: WHO (2009)
Healthcare workers • Specialist doctors • Medical Officers • Clinical Officers • Nurses • Public Health Officers
Major causes of morbidity • HIV/AIDS • Tuberculosis • Malaria • Pneumonia • Respiratory tract infections • Road accidents • Factory accidents • Gastroenteritis • Diabetes mellitus
Key Issues • A largely rural and poor population that has limited access to the formal healthcare system • Inadequate expenditure on health • No universal health financing scheme • Limited health workers; mostly urban based
CHW program in Loitokitok district Location • Kuku Group ranch – 1,500 sq.km • Semi-arid • Average Temp- 30 0 Celsius • 12,000 inhabitants - Maasai Community • Nomadic herders • Traditional
Implementing agencies/Institutions • Ministry of public health and sanitation • Maasai Trust • Christian Children’s Fund • African Medical Research Foundation (AMREF)
Health workers • Public health Officer (1) • Medical Officer (1) • Nurses (6) • Support staff (10)
Structure • CHW selection by community • Training (3 months) • Allocation • 1CHW per 2-3 homesteads (20-30 households) • Duties – Water, sanitation, ITNs, Immunization, Antenatal care, Delivery, nutrition, communicable diseases, health education • Resources – Bicycle, CHW bag, Stationery • Reporting/supervision • Monthly to health centre
Early challenges • Too much workload for CHWs • Motivation • Failure to translate theory into practice ? literacy • Large coverage area
Emergency measures • Reduce number of CHWs • Narrow focus • Closer supervision • Incentives
Notable successes • Increased immunization coverage • Home management of diarrhoea using Oral Rehydration Salts • Surveillance system
Failures • Water and Sanitation • Reproductive health • ITNs
Key Issues • Resource limited setting • Does it increase access? • Does it address health workers shortage? • Cost-effectiveness • Is it really cheap? • Empowering • Who decides? • Who acts? • How is success evaluated
Excerpts from Kenya budget 2011/2012 • £10m – Recruitment of 3,150 nurses and 1,050 public health officers for rural areas • £2.7m – 1,050 motorcycles and 2,100 CHWs in rural areas