Download
1 / 55
550 likes | 989 Views
Genetic Screening for Relatives of Hemochromatosis Patients. Resident Grand Rounds Dawn Graziano December 9, 2003. Case Presentation. PS is a 49 y/o female with DM dx’ed 1997 presents to clinic for f/u PMHx: DM, OA Meds: Glucophage, Tylenol

E N D
Genetic Screening for Relatives of Hemochromatosis Patients Resident Grand Rounds Dawn Graziano December 9, 2003
Case Presentation • PS is a 49 y/o female with DM dx’ed 1997 presents to clinic for f/u • PMHx: DM, OA • Meds: Glucophage, Tylenol • Social hx: 1 ½ ppd x 30 years. Denies EtOH, drugs. Lives with husband, daughter in W-S.
Case Presentation • Family hx: Father ↓ hemochromatosis, cirrhosis Mother ↑ COPD, Crohn’s Daugher ↑ DM Brother ↑ A&W Sister ↑ A&W
Given this patient’s history of hemochromatosis in a first degree relative, what testing, if any, is indicated?
Overview • Background • Study #1: Prevalence of Mutations • Study #2: Phenotypic Expression of Disease • Study #3: Cost Effectiveness Analysis of Screening for Hemochromatosis in Relatives • Return to Case Presentation • Conclusion
Review of Iron Overload • Normal iron content of body = 3-4 g • Hgb in circulating rbc’s = 2.5 g • Iron containing proteins = 400 mg • Iron bound to transferrin in plasma = 3-7 mg • Storage iron (ferritin or hemosiderin) • Adult men: 1 g • Adult women: less storage, but depends on menses/pregnancies/lactation/iron intake
Review of Iron Overload • No regulated mechanism of iron loss • Iron is lost in sweat/shed skin cells/GI losses (1 mg/d) • Premenopausal women lose 0.5 – 1 mg/d 2 menses
Review of Iron Overload • As iron increases, iron saturation of transferrin increases and iron is offloaded to cells with high levels of transferrin receptors heart liver thyroid gonads pancreas
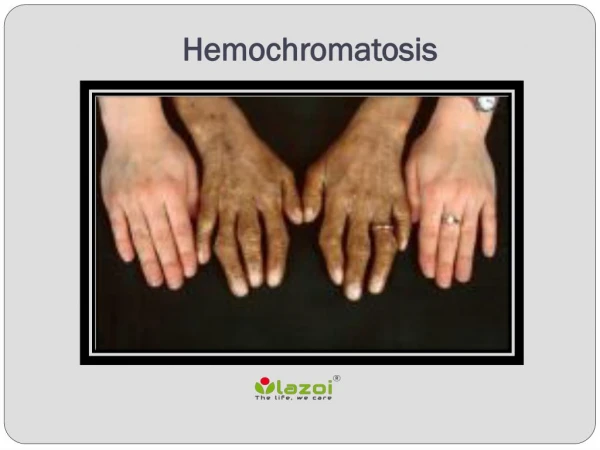
Review of Iron Overload • Clinical Presentation • Early sx’s: fatigue, impotence, arthralgia, arthritis, ↑LFT’s, abdominal pain, hepatomegaly • Late sx’s: skin bronzing, arthropathy, cardiomyopathy, DM, cirrhosis
Hereditary Hemochromatosis 2 Iron Overload Anemias Thalassemia major Sideroblastic Anemia Chronic hemolytic anemias Dietary iron overload Chronic Liver Disease Hep C, B EtOH induced liver dz Porphyria cutanea tarda Fatty liver dz Miscellaneous African iron overload Neonatal iron overload Aceruloplasminemia Congenital atransferrinemia Causes of Iron Overload
Diagnosis of Iron Overload • ↑ plasma iron conc (nl 60-150 µg/dL) • ↑ calculated transferrin sat (nl 20-45%) represents transport of excess iron from intestine • ↑ plasma ferritin (nl 40-200) represents iron accumulation in tissues
Diagnosis of Iron Overload • Traditionally, ↑ transferrin sat → repeat fasting trans sat + ferritin • Fasting trans sat > 45% identifies 98% of affected patients
Diagnosis of Iron Overload • Liver biopsy: • histologic eval, • hepatic iron concentration (HIC) • nl <36 µmol/g • >71 suggestive of hemochromatosis • hepatic iron index (HII) = HIC/age in years • If >1.9 virtually diagnostic of HH.
Hereditary Hemochromatosis • Autosomal recessive • ↑ intestinal iron absorption • Mutation(s) in HFE gene
HFE Genotype • C282Y: missense mutation leads to cytosine to tyrosine substitution at amino acid 282 • H63D: missense mutation leads to histidine to aspartate substitution at amino acid 63
HFE Genotype • 80% C282Y/C282Y • 4-7% compound heterozygotes (C282Y/H63D) • 3-10% C282Y/WT or H63D/WT (heterozygotes) • 1% H63D/H63D • 5-7% WT/WT
What is the prevalence of these genetic mutations in the U.S. population?
Prevalence of C282Y and H63D Mutations in HFE in the US, Steinberg, et al, JAMA, May 2001. Purpose: to estimate prevalence of HFE mutations in U.S. Design: cross-sectional population-based study of samples in DNA bank from phase 2 of NHANES III Genotypes 5171 specimens (>12 y/o, not pregnant, trans sat avail, did not list “other” as race/ethnicity)
Prevalence of C282Y and H63D Mutations in HFE in the US, Steinberg, et al, JAMA, May 2001. Results HFE GenotypePrev. Est. (95% CI) C282Y/C282Y 0.26 (0.12-0.49) H63D/H63D 1.89 (1.48-2.43) C282Y/H63D 1.97 (1.54-2.49) C282Y/WT 8.33 (7.45-9.33) H63D/WT 21.36 (20.02-67.76) WT/WT 66.20 (64.57-67.76)
Prevalence of C282Y and H63D Mutations in HFE in the US, Steinberg, et al, JAMA, May 2001. Results C282Y: 1 in 385 are homozygotes within previously published estimates of 1 in 200 to 1 in 500 No significant differences between men and women.
Prevalence of C282Y and H63D Mutations in HFE in the US, Steinberg, et al, JAMA, May 2001. • C282Y mutation estimated to be present in 5.4% of the total U.S. population • H63D mutation estimated to be present in 13.5% of the total U.S. population
Prevalence of C282Y and H63D Mutations in HFE in the US, Steinberg, et al, JAMA, May 2001. • Limits of Study • Powered only to estimate prevalence of homozygosity within total population (5171) • Randomly eliminated 20% of available subjects.
What proportion of homozygotes actually express the disease?
Disease-Related Conditions in Relatives of Patients with Hemochromatosis, Bulaj, et al, NEJM, November 2000. • Purpose: determine proportion of homozygotes with conditions related to hemochromatosis • 291 probands identified (184 presented with signs/symptoms of HH, 107 found because of transferrin sat at hemochromatosis screen or health maintenance) • 214 homozygous 1st degree relatives identified
Disease-Related Conditions in Relatives of Patients with Hemochromatosis, Bulaj, et al, NEJM, November 2000. • Homozygous relatives had iron profiles checked and were assessed for disease related conditions: • Cirrhosis • Hepatic fibrosis • Elevated LFT’s • Hemochromatic arthropathy
Disease-Related Conditions in Relatives of Patients with Hemochromatosis, Bulaj, et al, NEJM, November 2000. • Divided into 3 groups: • Iron overload with disease-related conditions • Iron overload without disease-related conditions • No iron overload
Disease-Related Conditions in Relatives of Patients with Hemochromatosis, Bulaj, et al, NEJM, November 2000. Results All ages: 38% of homozygous male relatives with at least 1 disease-related condition 10% of homozygous female relatives with at least 1 disease-related condition
Disease-Related Conditions in Relatives of Patients with Hemochromatosis, Bulaj, et al, NEJM, November 2000. Results Age-related: 52% of men with at least 1 disease-related condition by age 40 16% of women with at least 1 disease-related condition by age 50
Disease-Related Conditions in Relatives of Patients with Hemochromatosis, Bulaj, et al, NEJM, November 2000. • Limits of study: • Not all patients received gold standard of diagnosis (liver bx). Few female relatives (40/101) agreed to bx. • Only evaluated the C282Y/C282Y genotype
Why Screen for Hemochromatosis? • Prevalent disease • Long asymptomatic phase • Low risk, accessible treatment that prevents long-term sequelae of disease
Is there a cost-effective screening strategy for relatives of hemochromatosis patients? What is the role of genetic testing?
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. • Purpose: to compare the cost effectiveness of no screening with 4 different screening strategies, incorporating iron studies and genetic testing
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000.
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. 5 Strategies • No screening • Iron Studies • Gene test proband/spouse/children • Gene test proband/relatives • Gene test relatives
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. 1. No Screening Assumed 50% would develop organ damage cirrhosis DM cardiomyopathy
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. 2. Serum Iron Studies Measured serum transferrin and ferritin in children of proband starting at age 10, repeated for negative tests q5 yrs until age 40. Siblings were screened once.
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. 3. Gene test proband/spouse/children Proband tested. If homozygous, spouse tested. If spouse heterozygous, children tested. Homozygous children followed with iron studies as above.
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. 4. Gene test proband/relatives Proband tested. If homozygous, children and siblings tested. If relatives homozygous, iron studies. If proband not homozygous, children→periodic iron studies, siblings tested once with iron studies.
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. 5. Gene test relatives before proband Relatives gene tested. If homozygous → serum iron studies.
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. Screening Children If 1 child, gene testing proband, then child most cost effective ($508 per life-yr saved) If >1 child, gene testing proband, then spouse, then children most cost effective ($3665 per life-yr saved for 2 children) Serum iron studies: $7934 Relatives tested first: $12,277
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. Screening Siblings No screening: life expectancy 65 years All other strategies cost less & yielded greater benefit than no screening. 1 sibling: screening sibling 1st lower cost >1 sibling: gene testing proband 1st lower cost
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. Proportion of patients with phenotypic hemochromatosis in whom HFE test positive for C282Y/C282Y affects cost effectiveness. In this study, it was varied between 60-100%, testing proband/spouse/children cost effective. As it approaches 100%, gene testing relatives 1st becomes less expensive.
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. Recommendations Gene Test Proband If homozygous → gene test spouse → gene test siblings If spouse heterozygous → gene test children Iron studies in heterozygotes unnecessary.
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. Without gene testing, all 1st degree relatives would need iron studies until age 40 With gene testing: 95% of children and 75% of siblings spared further testing.
Screening for Hereditary Hemochromatosis in Siblings and Children of Affected Patients, El-Serag, et al, Annals of Int Med, February 2000. Limits of study • Cost of genetic testing assumed to be less than what is available at NCBH ($173 vs $245) and iron profile more ($85 vs $58) • Assumed higher percentage of patients with HH were homozygous for C282Y
Return to Case Presentation 49 year old female with family history significant for hemochromatosis in father. Told in the past, “my iron was high.”
Return to Case Presentation Labs iron 169 (40-160) transferrin sat 45% (15-45%) ferritin 305 (20-200) LFT’s wnl
Return to Case Presentation Genetic Testing C282Y: heterozygous H63D: not present