유방암의 Genetic Screening
유방암의 Genetic Screening. 영남의대 병리학교실 배 영 경. Breast cancer. Breast cancer susceptibility genes. * Breast cancer penetrance in mutation carriers. Problems in genetic screening of breast cancer. No unifying molecular alteration in sporadic breast cancer (genetically heterogeneous)

유방암의 Genetic Screening
E N D
Presentation Transcript
유방암의 Genetic Screening 영남의대 병리학교실 배 영 경
Breast cancer susceptibility genes *Breast cancer penetrance in mutation carriers
Problems in genetic screening of breast cancer • No unifying molecular alteration in sporadic breast cancer (genetically heterogeneous) • Low incidence of BRCA1/BRCA2 mutation in breast cancer • Large size of BRCA1/BRCA2 genes • No specific loci of mutation on BRCA1/BRCA2 genes • High cost: not covered by insurance • No domestic data of penetrance/cancer risk for BRCA1/BRCA2 mutation carriers
Germline mutation of BRCA1 & BRCA2 15-20% of familial breast cancer 5% of breast cancer overall
BRCA1 • Lifetime breast cancer risk: 60-80% • Lifetime ovarian cacner risk: 20-40% • Increased risk for prostate and colon cancer • Cell cycling, DNA-damage response
BRCA2 • Lifetime breast cancer risk: 60-85% • Lifetime ovarian cancer risk: 10-20% • Lifetime male breast cancer risk: 6% • Increased risk for colon, prostate, pancreas, GB, bile duct, stomach cancer and malignant melanoma • Maintenance of chromosome integrity
Cancer risk in women with germline BRCA1 mutations Nature Med 7: 552-6, 2001
Incidence of BRCA1/BRCA2 mutation • Non-cancer population Ashkenazi Jews: BRCA1: 1%, BRCA2: 1% General population: BRCA1: 0.06% • Breast cancer patients Unselected groups: BRCA1: 1.4%, BRCA2: 1.2% Early onset breast cancer patients (<45 yrs) BRCA1: 6-13% , BRCA2: 4-5% • Families with both breast and ovarian cancer BRCA1 &BRCA2: 55% • Families with both breast and ovarian cancer in the same individual BRCA1 &BRCA2: 75%
Incidence of BRCA1/BRCA2 mutation in Korean Breast Cancer *: High-risk patients with family history of breast or first-degree ovarian cancer, bilateral breast cancer, male breast cancer, multiple organ cancer, earlier age of onset(<35 yr). #: Early onset breast cancer patients: <40 yr
BRCA mutation carriers’ tumors • ER-negative • PR-negative • Cyclin D1-negative • HER-2/neu-negative • P53-positive • High nuclear and histologic grade
BRCA1-exon24 ‘ATTGGGCA’ deletion Analysis of BRCA1/BRCA2 mutation F-CSGE or DHPLC Direct sequencing
Limitation of widespread BRCA1/BRCA2 testing • Expensive cost • Uncertain clinical value of a positive test result • Fear of loss of health
Cost of genetic screening • 한국 요양급여비용의 100분의 100을 본인이 부담하는 항목 돌연변이검사 (확진) 121 다. 유전성유방암/난소암 BRCA1, BRCA2 305,740원 • 미국 $ 2400 – 2975 for both BRCA1 and BRCA2
Limitation of widespread BRCA1/BRCA2 testing • Expensive screening test • Uncertain clinical value of a positive test result • Fear of loss of health
Results of mutation analysis 1) Over 800 different mutations are found throughout the entire gene sequence 2) Nonsense or frame shift mutations protein truncation Missense mutation undetermined clinical significance 3) No founder mutations in Korean e.g.) Ashkenazi Jew, Iceland 4) No domestic data for penetrance of BRCA mutation
Cumulative risk of breast cancer by age in women from families with cancer-predisposing mutations Easton et al., 1995 and 1997
Limitation of widespread BRCA1/BRCA2 testing • Expensive cost • Uncertain clinical value of a positive test result • Fear of loss of health
Advantages to testing for BRCA mutations • Women may feel relieved knowing for certain whether or not they are at a higher risk for breast cancer. • Women with breast cancer may have better responses to certain treatments that are specifically designed for BRCA positive patients. • Women may take preventive measures to help reduce their risk of breast cancer if they are positive for BRCA mutations. • Other family members may decide if they wish to be tested for BRCA mutations based on the results of a woman’s test.
Disadvantages to testing for BRCA mutations • Women may become worried, panicked, or stressed if they discover they have a higher than average risk for breast cancer. • Women who test positive for BRCA mutations are faced with the difficulty of telling family members • Women who test negative for BRCA mutations may falsely believe they will never get breast cancer.
Genetic Screening • Who to screen • Who may not need screen • How reducing the incidence and morbidity of breast cancer • How reducing health care cost • How benefiting women, their families, and society
Models for prediction of BRCA1/BRCA2 mutations (by NCI) • Personal characteristics • Breast cancer diagnosed at an early age • Bilateral breast cancer • A history of both breast and ovarian cancer • The presence of breast cancer in 1 or more male family members • Family characteristics • Multiple cases of breast cancer in the family • Both breast and ovarian cancer in the family • One or more family members with 2 primary cancers • Ashkenazi Jewish background
Recommendation for BRCA mutation analysis High-risk patients with 1) family history of breast or first-degree ovarian cancer 2) bilateral breast cancer 3) male breast cancer 4) multiple organ cancer including breast cancer 5) earlier age of onset (<35 yr) Ahn et al. J Korean Med Sci 19: 269-74, 2004
Risk assessment of patients with a family history of breast cancer Warner E, et al. Canadian Family Physician 45: 105-112, 1999.
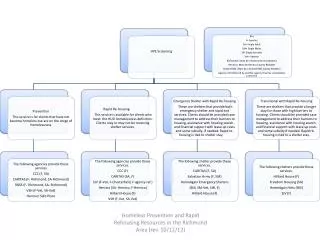
One FDR > 50yr, or More distant relative One FDR < 50yr, two FDRs or male relative Patient requests gene testing Inherited risk education or Genetic counseling No genetic risk or patient does not want gene testing Patient desires further gene testing negative Test for mutations in affected relatives Routine breast cancer surveillance positive negative Test for mutations in patient positive
positive Begin early surveillance program Age 18: monthly breast self-examinations Age 25: monthly breast self-examinations annual clinical examinations annual mammograms Prophylactic mastectomy after childbearing? For those with BRCA1 mutation, annual CA-125 and pelvic ultrasound examinations prophylactic oophorectomy after age 40? Suggested algorithm for genetic screening based on recommendations by the National Institutes of Health and the National Human Genome Research Institute.
The Johns Hopkins Breast and Ovarian Surveillance Service (BOSS) • review family history and other risk factors • provide individualized risk assessment • perform a clinical breast exam and instruct patients in breast self-exam • discuss and offer genetic testing to evaluate inherited cancer susceptibility • provide individualized cancer prevention and screening information • discuss the benefits and risks of hormone replacement therapy • provide information about chemoprevention of breast cancer in high risk women
What to do? • Select high-risk family • Genetic counselor • Give information for genetic testing • Explore the clinical significance of unverified mutations • Develop standardized protocol for genetic testing and follow-up of mutation carriers • Support the cost of genetic testing for the high-risk family