Live Donor Registry
110 likes | 218 Views
Explore data from the Live Donor Registry on kidney function, risks, and outcomes in live kidney donors, including GFR calculations, prevalence of abnormal glucose metabolism, and post-nephrectomy follow-up. Key issues such as ESKD frequency, mortality, and risk factors are analyzed.

Live Donor Registry
E N D
Presentation Transcript
Live Donor Registry Steve Chadban
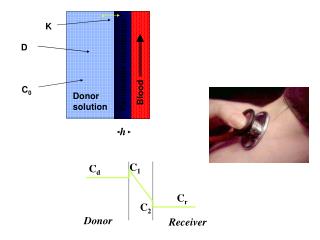
Impaired kidney function Calculated GFR (body surface area adjusted) Median and interquartile range
Prevalence of abnormal glucose metabolism* in Australian Adults, AusDiab 1999-2000. *WHO criteria after OGTT Dunstan etal. Diabetes Care 2002;25:829-34
Patients who have undergone unilateral nephrectomy who are obese: Praga et al. KI 2000;58:2111
Risk of ESKD after kidney donation - USA • Kidney donors on waiting list 0.15% • Incidence • white < 50 0.04% • Black <50 0.2% • Significantly greater than risk in age matched pop gen pop donor • White 30-39 0.008 0.1 • Black 0.04 0.52 • Cause of ESRF • FSGS • DM • 20-50% have a family Hx of DM • Age at donation 38.5y • Age at ESRF 49 Connie Davis, ATC 2005
Pre-donation data • Commenced 2004, data 2004-6 = 764 (>95%) • Age 48+/-11yrs, 25%>57, 18%>60 • F 56%, M 44%, 89% caucasian • 62% related, 22%spousal, 15% other LURD • SCr 78+/-15 umol/L, 25%>88 • GFR 112 +/-30, GFR<96 in 25% • Nuc GFR (n=329) 117+/-23, 25% <100, 2%<80 • MDRD or CrCl (n=250) 107 +/-36, 25%<76, 29%<80
Pre-donation data • SCr 78+/-15 umol/L, 25%>88 • GFR 112 +/-30, GFR<96 in 25% • Nuc GFR (n=329) 117+/-23, 25% <100, 2%<80 • MDRD or CrCl (n=250) 107 +/-36, 25%<76, 29%<80 • Proteinuria (n=627 or 82%) • Mean 0.12g/day • >0.20g/d in 21 (3.3%)
Pre-donation data • BMI 26 +/-4.0 – 16% 30-35, 2.3% > 35 • Diabetes – known (10) + OGTT (14) = 24 (3%) • OGTT reported 70%, 81% normal, 17% IFG, 2% DM • +FHx in 21% • 2 diabetic donors with BP>140/90 • BP 125/75 +/- 13/9 • Systolic BP >140 in 6%, DBP >90 in 2.7%, >140/90 in 1.6% • Smoking – 8.3%
Follow-up post-nephrectomy • 1 year = 23%, 2 year = 15% • 1yr follow-up (n=235): • SBP 124±13 • DBP 75±8 • New hypertension 10% • SCr 108±23 • MDRD 59±12 – 25% <51 • PCR (n=75) 5.6±5.5 • Reported problems (n) – elevated SCr (6), proteinuria (3), pain (1), IgA (1), retroperitoneal fibrosis (1).
Key Issues Follow-up – non-mandated but crucial! • Current follow-up data not useful • Frequency of ESKD among donors, mortality • Outcomes at extremes of GFR • Hyperfiltration – GFR>140 with low-grade proteinuria • Low baseline GFR – typically elderly, impact on CVS outcomes • Proteinuria – development, evolution, relationship to BMI, diabetes • BP – kidney, CVS and BP outcomes among hypertensives, smokers • Controls