Download
1 / 42
420 likes | 468 Views
Join Dr. Selim Krim, MD, Assistant Professor at Texas Tech University, for a step-by-step ECG interpretation lecture. Learn about heart rate, rhythm analysis, conduction abnormalities, and waveform description. Understand how to calculate heart rate and identify abnormalities in P waves, QRS complexes, ST segments, T waves, and U waves. Practice your ECG interpretation skills and compare with previous ECGs. Perfect for medical students and healthcare professionals! ###

E N D
ECG Lecture Part 1 ECG Interpretation Selim Krim, MD Assistant Professor Texas Tech University Health Sciences Center
Step wise approach to ECG • Measurements • Rhythm Analysis • Conduction Analysis • Waveform Description • ECG Interpretation • Comparison with Previous ECG (if any)
Measurements • Heart rate 60-90 bpm • PR interval (from beginning of P to beginning of QRS) =0.12-0.20 sec • QRS duration (width of most representative QRS) <0.12 sec • QT interval (from beginning of QRS to end of T) = 0.42 sec • QRS axis in frontal plane
Heart rate • State atrial and ventricular rate. • P wave rate 60-100 bpm • Rate < 60 = Sinus bradycardia • Rate > 90 = Sinus tachycardia
How to calculate Heart Rate • Standard textbooks of physiology and medicine mention that heart rate (HR) is readily calculated from the ECG as follows: HR = 1,500/RR interval in millimeters, HR = 60/RR interval in seconds, or HR = 300/number of large squares between successive R waves
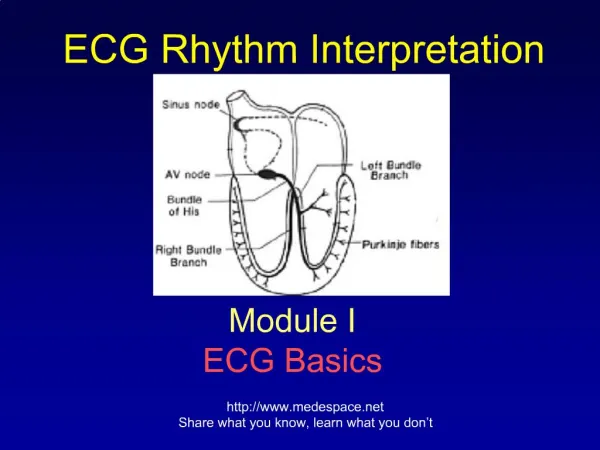
The P wave represents atrial activation; the PR interval is the time from onset of atrial activation to onset of ventricular activation. The QRS complex represents ventricular activation; the QRS duration is the duration of ventricular activation. The ST-T wave represents ventricular repolarization. The QT interval is the duration of ventricular activation and recovery. The U wave probably represents "after depolarizations" in the ventricles.
Step wise approach to ECG • Measurements • Rhythm Analysis • Conduction Analysis • Waveform Description • ECG Interpretation • Comparison with Previous ECG (if any)
Rhythm Analysis • State basic rhythm (e.g., "normal sinus rhythm", "atrial fibrillation", etc.) • Identify additional rhythm events if present (e.g., "PVC's", "PAC's", etc) • Consider all rhythm events from atria, AV junction, and ventricles
Rhythm Analysis Sinus rhythm defined as; • Each P wave is followed by QRS • P wave is positive in lead I, II • Constant PR interval
Step wise approach to ECG • Measurements • Rhythm Analysis • Conduction Analysis • Waveform Description • ECG Interpretation • Comparison with Previous ECG (if any)
Conduction Analysis • Sino-Atrial Exit Block (SA Block): Type 1,2 • Atrio-Ventricular (AV) Block: 1st, 2nd and 3rd degree • AV Dissociation • Intraventricular Blocks; RBBB, LBBB, LAFB, RPFB, Bifascicular • Nonspecific Intraventricular Conduction Defects (IVCD) • Wolff-Parkinson-White Preexcitation
Step wise approach to ECG • Measurements • Rhythm Analysis • Conduction Analysis • Waveform Description • ECG Interpretation • Comparison with Previous ECG (if any)
Waveform Description • Carefully analyze the 12-lead ECG for abnormalities in each of the waveforms in the order in which they appear: • P waves: are they too wide, too tall, look funny (i.e., are they ectopic), etc.? • QRS complexes: look for pathologic Q waves, abnormal voltage, etc. • ST segments: look for abnormal ST elevation and/or depression. • T waves: look for abnormally inverted T waves. • U waves: look for prominent or inverted U waves.
The normal U wave has the same polarity as the T wave and is usually less than one-third the amplitude of the T wave. U waves are usually best seen in the right precordial leads especially V2 and V3. The normal U wave is asymmetric with the ascending limb moving more rapidly than the descending limb (just the opposite of the normal T wave).
Step wise approach to ECG • Measurements • Rhythm Analysis • Conduction Analysis • Waveform Description • ECG Interpretation • Comparison with Previous ECG (if any)
ECG Interpretation • This is the conclusion of the above analyses. Interpret the ECG as "Normal", or "Abnormal". Occasionally the term "borderline" is used if unsure about the significance of certain findings. List all abnormalities. Examples of "abnormal" statements are: Inferior MI, probably acute • Old anteroseptal MI • Left anterior fascicular block (LAFB) • Left ventricular hypertrophy (LVH) • Nonspecific ST-T wave abnormalities • Any rhythm abnormalities
Step wise approach to ECG • Measurements • Rhythm Analysis • Conduction Analysis • Waveform Description • ECG Interpretation • Comparison with Previous ECG (if any)