ECG interpretation
ECG interpretation. Dr Ally Duncan SpR In Anaesthesia & Clinical Fellow in Undergraduate Medical Education Manchester Royal Infirmary May 2012. Objectives. Justify the reasons for performing an ECG Develop a structured approach to interpreting an ECG Practice interpreting ECGs. The ECG.


ECG interpretation
E N D
Presentation Transcript
ECG interpretation Dr Ally Duncan SpR In Anaesthesia & Clinical Fellow in Undergraduate Medical Education Manchester Royal Infirmary May 2012
Objectives • Justify the reasons for performing an ECG • Develop a structured approach to interpreting an ECG • Practice interpreting ECGs
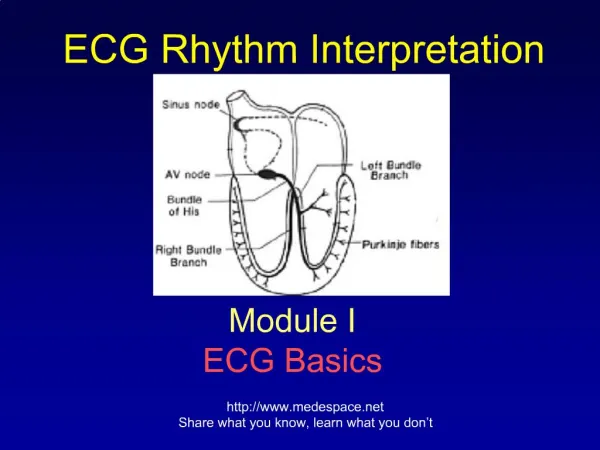
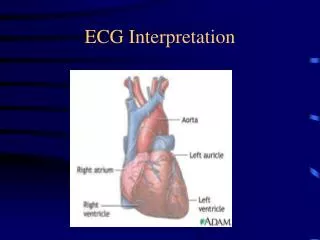
The ECG “The ECG (electrocardiogram) is a transthoracic interpretation of the electrical activity of the heart.”
Why perform an ECG? • It’s part of the admission bundle • Indicated by the patient’s symptoms - symptoms of IHD/MI - symptoms associated with dysrhythmias • Indicated by the patient’s examination findings - cardiac murmur
Quality of ECG? Rate Rhythm Axis P wave PR interval QRS duration QRS morphology Abnormal Q waves ST segment T wave QT interval ECG interpretation
Quality of the ECG • Patient name • Date of the ECG • Is there any interference? • Is there electrical activity from all 12 leads? • Calibration: - speed = 25mm/second - height = 1cm/mV
ECG interpretation • Quality of ECG? • Rate • Rhythm • Axis • P wave • PR interval • QRS duration • QRS morphology • Abnormal Q waves • ST segment • T wave • QT interval
Rate • 300/number of big squares between R waves • Rate is either: - normal - bradycardic - tachycardic
Rhythm • Are there P waves? • Are they regular? • Does one precede every QRS complex? • Regular vs. irregular
Axis Positive in I and II = NORMAL Positive in I and negative in II = LAD Negative in I and positive in II = RAD
ECG interpretation • Quality of ECG? • Rate • Rhythm • Axis • P wave • PR interval • QRS duration • QRS morphology • Abnormal Q waves • ST segment • T wave • QT interval
P wave • Are there P waves present? • Bifid = P mitrale (LA hypertrophy) • Pointy = P pulmonale (RA hypertrophy)
PR interval • Start of P wave to start of QRS complex • Normal = 0.12 - 0.2 seconds (3-5 small squares) • Decreased = can indicate an accessory pathway • Increased = indicates AV block (1st/2nd/3rd)
ECG interpretation • Quality of ECG? • Rate • Rhythm • Axis • P wave • PR interval • QRS duration • QRS morphology • Abnormal Q waves • ST segment • T wave • QT interval
QRS complex • Normal = <0.12 seconds • >0.12 seconds = Bundle Branch Block
QRS complex W I LL ia m = LBBB M a RR o w = RBBB
QRS complex • Is there LVH? • Sum of the Q or S wave in V1 and the tallest R wave in V5 or V6 >35mm is suggestive of LVH
Q waves • Q waves are allowed in V1, aVR & III • Pathological Q waves can indicate previous MI
ECG interpretation • Quality of ECG? • Rate • Rhythm • Axis • P wave • PR interval • QRS duration • QRS morphology • Abnormal Q waves • ST segment • T wave • QT interval
ST segment • ST depression - downsloping or horizontal = ABNORMAL • ST elevation - infarction - pericarditis (widespread)
T wave • Small = hypokalaemia • Tall = hyperkalaemia • Inverted/biphasic = ischaemia/previous infarct
QT interval • Start of QRS to end of T wave • Needs to be corrected for HR • Normal QTc = < 400ms • Long QT can be genetic or iatrogenic
Summary • Discussed the indications for performing an ECG • Introduced an approach to interpreting ECGs • Discussed common ECG abnormalities