Download
1 / 28
400 likes | 1.05k Views
Hypothalamus & Pituitary Gland. Hypothalamus and Pituitary Gland. The hypothalamus and pituitary gland form a unit that exerts control over the function of several endocrine glands (thyroid, adrenals, and gonads), as well as a wide range of physiologic activities

E N D
Hypothalamus and Pituitary Gland The hypothalamus and pituitary gland form a unit that exerts control over the function of several endocrine glands (thyroid, adrenals, and gonads), as well as a wide range of physiologic activities This unit constitutes an example of neuroendocrinology—brain-endocrine interactions
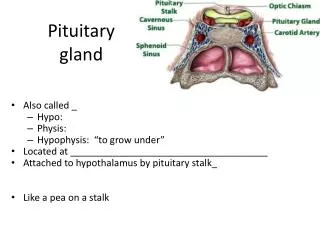
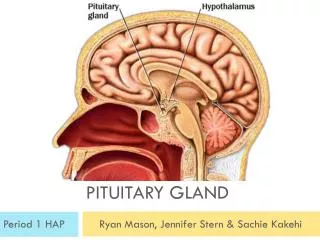
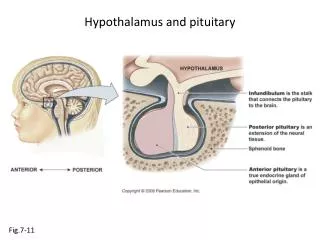
Morphology Sellaturcica The pituitary gland (hypophysis) is located in a small depression in the sphenoid bone, the sellaturcica, just beneath the hypothalamus It is connected to the hypothalamus by a thin stalk called the infundibulum
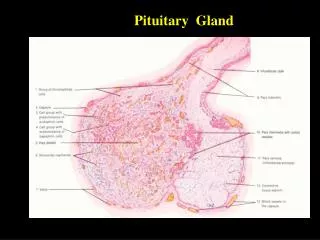
Histology of the Anterior Lobe Most of the cells in the anterior lobe (adenohypophysis) contain secretory granules, although some are only sparsely granulated Based on their characteristic staining with standard histochemical dyes and immunofluorescent stains, it is possible to identify the cells that secrete each of the pituitary hormones It once was thought that there was a unique cell type for each of the pituitary hormones, but it is now recognized that some cells may produce more than one hormone
Histology of the Posterior Lobe • The posterior lobe (neurohypophysis) consists of two major portions: • the infundibulum, or stalk, • and the infundibularprocess, or neural lobe • The posterior lobe is richly endowed with fibers • The cell bodies from which these fibers arise are located in the hypothalamus • Secretory material synthesized in cell bodies in the hypothalamus is transported down the axons and stored in in the posterior lobe
Physiology of the Anterior Pituitary Gland • There are six anterior pituitary hormones whose physiological importance is clearly established • They include the hormones that govern the function of the: • thyroid and adrenal glands, • the gonads, • the mammary glands, • and bodily growth
Hormones of the Anterior Pituitary Gland • All the anterior pituitary hormones are proteins or glycoproteins • They are divided into 3 categories according to structure similarity: • Glycoprotein Hormones • Growth hormone and prolactin • Adrenocorticotropin family
Growth Hormone and Prolactin Somatotropes (GH producing cells) are by far the most abundant anterior pituitary cells, and account for at least half the cells Structurally, prolactin (PRL) is closely related to GH
AdrenocorticotropinFamily • The ACTH related peptides constitute a family because: • they contain regions of homologous amino acid sequences, which may have arisen through exon duplication, • and because they all are encoded in the same gene
Regulation of Anterior Pituitary Function • Secretion of the anterior pituitary hormones is regulated by: • the central nervous system • provides the primary drive for secretion • and hormones produced in peripheral target glands • and peripheral input plays a secondary, though vital, role in modulating secretory rates • Secretion of all the anterior pituitary hormones except PRL declines severely in the absence of stimulation from the hypothalamus as can be produced • when the pituitary gland is removed surgically from its natural location and reimplanted at a site remote from the hypothalamus • PRL secretion is normally under tonic inhibitory control by the hypothalamus
Feedback Control of Anterior Pituitary Function • Environmental factors may increase or decrease pituitary activity by increasing or decreasing hormone secretions from hypothalamus • Pituitary secretions increase the secretion of target gland hormones, which may inhibit further secretion by acting at either the hypothalamus or the pituitary • Pituitary hormones may also inhibit their own secretion by a short feedback loop
Physiology of the Posterior Pituitary • The posterior pituitary gland secretes two hormoneswhich are: • oxytocin , • increase uterine contractions during parturition • Contraction of mammary glands to secret milk • and vasopressin or arginine vasopressin (AVP) (or Antidiuretic Hormone ‘ADH’) • contract vascular smooth muscle and thus raise blood pressure • promote reabsorption of water by renal tubules
Physiology of the Posterior Pituitary Oxytocin and AVP are stored in and secreted by the posterior pituitary gland, but are synthesized by the hypothalamus
Regulation of Posterior Pituitary Function Regulation of oxytocin secretion showing a positive feedback arrangement. Increased blood osmolality or decreased blood volume are sensed in the brain or thorax, respectively, and increase vasopressin secretion.
Hypophysiotropic hormones Physiological actions of the pituitary Hormone
Pituitary & Hypothalamic Disorders • Hypothalamic-pituitary lesions present with a variety of signs, including pituitary hormone: • hypersecretionand hyposecretion, • sellarenlargement, • and visual loss
Pituitary & Hypothalamic Disorders • In adults, the most common cause of hypothalamic-pituitary dysfunction is a pituitary adenoma, of which the great majority are hypersecreting • Thus, the earliest symptoms of such tumors are due to endocrinologic abnormalities and include: • Early manifestation • Hypogonadism, the most frequent • diminished functional activity of the gonads • Late manifestation in patients with larger tumors or suprasellar extension • sellar enlargement • headache • and visual loss,
GonadotrophinsDisorders • Hyposecretion • leads to amenorrhoea, • sterility • and loss of sexual potency. • In the young, the sex organs and secondary sexual characteristics fail to develop (delayed puberty) • Hypersecretion • extremely rare, • in children it could lead to sexual precocity (excessive premature development)
ThyrotrophinDisorders • Hyposecretion • produces a clinical picture similar to primary thyroid deficiency • Hypersecretion • gives the symptoms of hyperthyroidism similar to Graves’ disease
Corticotrophin Disorders • Hyposecretion • rare • causes failure of cortisol secretion, • a general lack of health and well being, • a reduced response to stress and skin depigmentation • Hypersecretion • due to a pituitary microadenoma, • will result in Cushing’s syndrome
Prolactin Disorders • Hyposecretion • leads to failure of lactation in women • Hypersecretion • may result from a pituitary tumour • principal symptoms are infertility and menstrual complaints • in men, decreased libido, • inadequate sperm production and impotence, whereas in women, there may be a complete lack of menstruation • inappropriate (non-pregnant) milk production
GHRH Disorders • Hyposecretion • caused by hypothalamic or pituitary dysfunction • In childhood this leads to impairment of growth (dwarfism) • Hypersecretion • This usually results from a benign pituitary tumour • In young patients, this leads to gigantism • In adults, leads to acromegaly
Vasopressin Disorders • Hyposecretion • caused by damage or dysfunction of the hypothalamus, • can lead to diabetes insipidus, • excessively large amounts of dilute urine (10–15 liters/day) are produced by the kidneys • Hypersecretion • rare condition of inappropriate AVP production is known as syndrome of inappropriate ADH(SIADH)
Hypopituitarism • Hypopituitarism is manifested by diminished or absent secretion of one or more pituitary hormones • Hypopituitarism is either: • a primary event • caused by destruction of the anterior pituitary gland • or a secondary phenomenon • resulting from deficiency of hypothalamic stimulatory factors normally acting on the pituitary
Assessment of Target Gland Function • If endocrine hypofunction is suspected, pituitary hormone deficiencies must be distinguished from primary failure of the thyroid, adrenals, or gonads • Baseline laboratory studies should include: • thyroid function tests (free T4) • and determination of serum testosterone levels • Testosterone is a sensitive indicator of hypopituitarism in women as well as in men
In primary target gland hypofunction, such as autoimmune polyglandular syndromes types 1 and 2 (APS 1 and 2), TSH, LH, FSH, or ACTH will be elevated Low or normal values for these pituitary hormones suggest hypothalamic-pituitary dysfunction