Download
1 / 37
530 likes | 1.55k Views
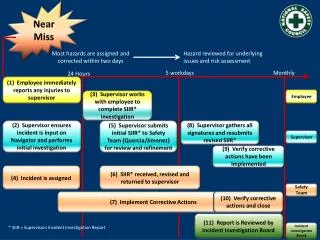
MATERNAL NEAR MISS AT HOLY FAMILY HOSPITAL Prof. Fehmida Shaheen Head of Obs/Gynae Unit-II Holy family Hospital, Rawalpindi. Maternal mortality is “Just the tip of iceberg” has vast base to the iceberg maternal morbidity which remains undescribed. Maternal Mortality.

E N D
MATERNAL NEAR MISS AT HOLY FAMILY HOSPITAL Prof. Fehmida Shaheen Head of Obs/Gynae Unit-II Holy family Hospital, Rawalpindi
Maternal mortality is “Just the tip of iceberg” has vast base to the iceberg maternal morbidity which remains undescribed.
Maternal Mortality Severe Maternal Morbidity
“A maternal near-miss case “a woman who nearly died but survived a complication that occurred during pregnancy, childbirth or within 42 days of termination of pregnancy” In practical terms, “women are considered near miss cases when they survive life-threatening conditions (i.e. organ dysfunction)”. A very ill woman who would have died had it not been that luck and good care was on her side.
Why Maternal Near Miss? • Two decades age, in low maternal mortality setting, Morbidity useful indicator of obstetrics care. • In recent years analyzing near miss cases understanding health system failures in relation to obstetrics care
Why Maternal Near Miss? • Near miss cases share many characteristics with maternal deaths and can directly inform on obstacles that had to be overcome after the onset of an acute complication. • Corrective actions for identified problems can be taken to reduce related mortality and long-term morbidity.
Concept of Maternal Near Miss For last 20 years it has been explored in maternal health • As an adjunct to maternal death confidential inquiries • Have been studied as surrogates of maternal deaths
The WHO Maternal Near Miss Approach • A benchmark practice for monitoring maternal health care • Criteria for diagnosis of maternal near miss has been standardized “WHO. Evaluating the quality of care for severe pregnancy complications: the WHO near-miss approach for maternal health. Geneva: WHO, 2011”
WHO set of Severity Markers used in maternal near miss assessments
Benefit of setting the criteria for diagnosis of maternal near miss • Common ground for implementation of near miss assessments across countries • Allows international comparisons to be carried out
Objective of Our Study To determine the : • Frequency of maternal near miss, MNM Incidence Ratio (MNMIR) and mortality index • Analyze the nature of maternal near miss events • To compare the causes of maternal near miss with that of maternal mortality
Material and Methods Place of study: Gynae Unit II Holy Family Hospital, Rawalpindi Duration of Study: 1st Jan 2012 To 31st Oct 2013
Holy Family Hospital Provides • Antenatal care • Delivery services to both high and low risk pregnant women • 24hours emergency obstetric services • 24hours blood bank facility • Blood component therapy (available during morning hours only) • Surgical and medical intensive care units (ICUs)
Selection Criteria • Maternal near miss cases were selected which met WHO 2009 criteria (a set of clinical, laboratory and management based criteria) • Maternal mortality during the study period was analyzed • Patient characteristics including age, parity, gestational age at admission and surgical intervention to save the life of mother were considered
Maternal near miss and maternal mortality cases All were categorized by final diagnosis with respect to • Direct causes ( hypertension, hemorrhage, sepsis etc.) • Indirect causes (anemia, cardiac disease etc.)
Maternal Near Miss Indices • MNM Incidence Ratio (MNMIR = MNM/1000 live births) • Maternal near miss and mortality ratio (MNM : MD) • Mortality index ([MD/MNM +MD]×100)
Results Study Period: 1st Jan 2012 to 31st Oct 2013 Total live births 15,757 Total maternal near miss cases 198 Total maternal deaths 49
Characteristic of Maternal Near Miss Cases and Maternal Deaths
Comparison of near miss events and primary causes of maternal deaths
Surgical Intervention in Near Miss Cases to Save Life (n=89)
WHO Criteria 2009 • Incorporates both mantel’s and waterston criteria • Minimizes the chance of missing the case. • (M. Waterstone, C. Wolfe, and S. Bewley, “Incidence and pre-dictors of severe obstetric morbidity: case-controlstudy,” British Medical Journal, vol. 322, no. 7294, pp. 1089–1093, 2001.)
MNM incidence ratio in our study: 12.5/1000 live births Comparable to studies in developing countries Same trend vary between 15-40 / 1000 live births. However various criteria for identifying the cases were used. (J. van Roosmalen and J. Zwart, “Severe acute maternal morbidity in high-income countries,” Best Practice and Research: Clinical Obstetrics and Gynaecology, vol. 23, no. 3, pp. 297–304, 2009).
Our MNMIR 12.5 / 1000 live births Study from Brazil 4.4 / 1000 live births (in an intensive care unit) Study from India 17.8 / 1000 live birth F. A. Lotufo, M. A. Parpinelli, S. M. Haddad, F. G. Surita, and J. G. Cecatti, “Applying the new concept of maternal near-miss in an intensive care unit,” Clinics, vol. 67, no. 3, pp. 225–230, 2012. Roopa PS, ShailjaVerma, Lavanya Rai, Pratap Kumar, Murlidhar V. Pai, JyothiShetty. “Near Miss’’ Obstetric Events and Maternal Deaths in a Tertiary Care Hospital: An Audit. Hindawi Publishing Corporation Journal of Pregnancy Volume 2013, Article ID 393758, 5 pages http://dx.doi.org/10.1155/2013/393758
Maternal Mortality Ratio During the study period 310 / 100,000 live births Indian study 313 / 100,000 live births (Roopa PS, ShailjaVerma, Lavanya Rai, Pratap Kumar, Murlidhar V. Pai, JyothiShetty. “Near Miss’’ Obstetric Events and Maternal Deaths in a Tertiary Care Hospital: An Audit. Hindawi Publishing Corporation Journal of Pregnancy Volume 2013, Article ID 393758, 5 pages http://dx.doi.org/10.1155/2013/393758) Brazilian Study 51.6/100,000 live births (for the institution) (F. A. Lotufo, M. A. Parpinelli, S. M. Haddad, F. G. Surita, and J. G. Cecatti, “Applying the new concept of maternal near-miss in an intensive care unit,” Clinics, vol. 67, no. 3, pp. 225–230, 2012).
Characteristics of Cases in Both Groups • Non booked • Late referral • Multiple seizures before admission in cases of eclampsia
Study from Brazil • Main determinant of Maternal Near Miss • Hypertensive disorders but no death • (probably appropriate intervention in an adequate time frame) • “(F. A. Lotufo, M. A. Parpinelli, S. M. Haddad, F. G. Surita, and J. G. Cecatti, “Applying the new concept of maternal near-miss in an intensive care unit,” Clinics, vol. 67, no. 3, pp. 225–230, 2012).”
Sepsis • In our study MNMIR 0.5 / 1000 live births • Developed countries MNMIR 0.2 / 1000 live births
Maternal Near Miss To Mortality Ratio MNM:MD • In our study 4 : 1 • Study from Nepal 7.2 : 1 • Syrian study 60 : 1 • High income countries 117-223 : 1
Limitations ofOur Study • Retrospective analysis • In a single unit • However • New WHO criteria applied for maternal near miss cases
Conclusion • Maternal Near Miss Analysis Provide information • About obstacles leading to maternal near miss (inadequate care at primary level, failure to anticipate or diagnose the problem leading to late referral). • Inappropriate or inadequate management of maternal near miss cases (poor resources, inadequate utilization of resources at tertiary level). • NEAR MISS ANALYSIS IS WORTH PRESENTING IN NATIONAL INDICES.
Mother Tragedies are always in her path and its our responsibility to give her a safe motherhood