Download
1 / 37
370 likes | 620 Views
Development Considerations for Cell & Tissue Therapies and Gene Therapies. Elizabeth Read, MD Epi 260 UCSF May 9, 2012. Cell & Tissue Therapies. Development pathway for 351 HCT/Ps (same as drugs & conventional biologics). How HCT/Ps differ as a product class. Extremely heterogeneous

E N D
Development Considerations forCell & Tissue TherapiesandGene Therapies Elizabeth Read, MD Epi 260 UCSF May 9, 2012
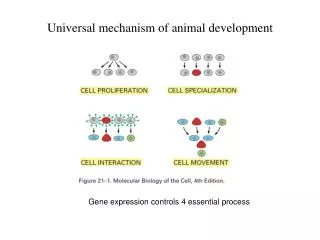
Development pathway for 351 HCT/Ps (same as drugs & conventional biologics)
How HCT/Ps differ as a product class • Extremely heterogeneous • Unique manufacturing & characterization challenges, related to • Human donor source: autologous vs. allogeneic related vs. allogeneic unrelated “off the shelf” • Multiple cell populations (in many products) • Can’t use terminal sterilization • Living cells are inherently unstable • Unusual routes of administration • FDA regulations, guidance, and review approaches have evolved relatively recently
Few HCT/Ps are currently licensed(list below current as of June 2011)
HCT/Ps licensed since June 2011 • Azficel-T (Fibrocell Technologies) – June 2011 • Autologous fibroblasts, for nasolabial fold wrinkles • Hemacord (NY Blood Center) – Nov 2011 • Allogeneic cord blood, for hematologic malignancies and other disorders • GINTUIT (Organogenesis) – Mar 2012 • Allogeneic cultured keratinocytes and fibroblasts in bovine collagen, for mucogingival conditions
Approved cell therapies in context of other approved biologics Kozlowski et al. NEJM 2011
Additional CMC Guidances DISEASE/PRODUCT-SPECIFIC • Cellular therapies for cardiac disease (Final guidance, Oct 2010) • Therapeutic cancer vaccines (Draft guidance, Sept 2009) • Considerations for allogeneic pancreatic islet cell products (Final guidance, Sept 2009) • Considerations for IDEs/INDs for products to repair/replace knee cartilage (Draft guidance, Jul 2007) • Cord blood for hematopoietic reconstitution for specified indications (IND and BLA guidances 2009) ASSAYS • Potency tests for cellular and gene therapy products (Final guidance, Jan 2011) • Validation of growth-based rapid micro methods for sterility testing (Draft guidance, Feb 2008)
CMC development issues:Cell Source • Need to assess effect of biological variability on manufacturing process steps • For autologous products, cell source from diseased patients may not be readily available for development • Therefore, may need to assess & demonstrate comparability between normal and patient-sourced cells/tissue
CMC development issues:Manufacturing Steps • Most manufacturing steps, including efforts to improve purity of cell populations, result in cell losses • Tech transfer from research to clinical manufacturing (including use of clinical grade containers and reagents) is often not straightforward
Graft Engineering for Hematopoietic Transplant4 log depletion of T cells in PBSC product at clinical scale predictably eliminated CD3+ T cells, but resulted in 50% loss of CD34+ cells CD34:CD3 = 100:1 CD34:CD3 = 1:50 CD34 CD3 Before After
Containers for Dendritic Cells Maturation of immature dendritic cells (DCs) in polystyrene (PS) flasks vs. teflon (FEP) bags resulted in different morphology, phenotype, and in vitro function. R Kurlander et al. 2006
CMC development issues:Hold/Storage/Stability • For many products, coordination of donor collection, manufacturing, and product administration is difficult and/or you may want to create inventory of products • Therefore, may need to cryopreserve starting cell source, intermediate products, or final products • Cryopreservation has consequences for product quality and feasibility of product administration at clinical sites
CMC development issues:Characterization & Potency Assays FDA Guidance (2011) • “Ideally, the potency assay will represent the product's mechanism of action …” • “However, many CGT products have complex and/or not fully characterized mechanisms of action, making it difficult to determine which product attributes are most relevant to measuring potency.”
CMC development issues:Tissue Engineering: Developing aCell + Scaffold Combination Product
Preclinical animal studies for HCT/Ps • CBER Office of Cellular, Tissue, and Gene Therapies (OCTGT) Pharm/Tox group • Case-by-case approach • Encourages informal pre-pre-IND meetings, and interactive planning and review of preclinical studies • Dec 2010 FR notice stated intent to write guidance on preclinical animal studies
Preclinical POC, PK/PD • Animal models of human disease/injury • Emphasis on biodistribution • In vivo survival, proliferation, differentiation, engraftment (what is desirable vs not?) • Migration to target & non-target sites • Monitor cell trafficking by terminal and non-terminal methods • Emphasis on ROA - feasibility & optimization
Animal Model Challenges • Choice of animal models • Many models are novel and/or have limitations • FDA usually asks for large animal to model aspects of delivery and biodistribution, permit higher cell doses • Xeno immune response to human cells complicates study • Immuno-incompetent mouse model vs immuno-suppressed large animal – neither is ideal • Evaluate analogous cells in given species? • POC, PK/PD vs. Safety/Tox • FDA often recommends “hybrid” POC/Safety studies using animal model of human disease, because biodistribution/cell fate likely to be different in diseased animals and may affect safety endpoints
Preclinical safety endpoints forstem cell therapies • Implant site reaction • Inflammatory response in target & non-target tissue • Host immune response • Morphologic alterations in target & non-target tissues • Cell survival post transplantation • Cell migration/homing • Cellular fate-plasticity: differentiation, transdifferentiation, fusion • Integration into host tissue • TUMORIGENICITY • NOTE: ICH guidelines for testing reproductive toxicity, genotoxicity, and carcinogenicity typically do not apply
Clinical Protocol • Overall study design, patient population, endpoints not really different from drug trials • Dosing & dose escalation – may not be able to discern MTD, but may identify maximum feasible dose • Some clinical protocol issues addressed in CBER product/disease-specific guidances for cell therapies • Cardiac disease • Therapeutic cancer vaccines • Allogeneic pancreatic islet cell products • Repair/replacement of knee cartilage
Clinical Protocol: How are stem cell trials different? • For novel stem cell products, risk : benefit assessment is difficult • Rationale for clinical trial must be justified by especially strong proof of concept • Greater emphasis placed on product characterization and preclinical testing
Gene Therapy Approaches • In vivo • Vector containing gene sequences of interest administered directly to patient, designed to target certain cells/tissues • Regulated like other biologics/biotechnology products, plus FDA gene therapy guidances • Ex vivo • Cells genetically modified by vector ex vivo are administered to patient • Regulated like other HCT/Ps, plus FDA gene therapy guidances
Vectors for Gene Transfer • Vector = an agent used to introduce genetic material into cells • Vectors can be • viral (e.g., gamma retroviral, lentiviral, adenoviral, etc) • non-viral (e.g., plasmid DNA, liposomes) • Vector technology & transduction methods improving • enhance appropriate gene expression • Improve gene transfer efficiency • Novel approaches • Sangamo’s gene “editing” technology (zinc finger nucleases)
History of Gene Therapy Clinical Trials • 1974: NIH established Recombinant DNA Advisory Committee (RAC) • NIH Guidelines on recombinant DNA research • 1980s: New subcommittee of RAC to oversee clinical gene therapy • Appendix M to NIH Guidelines – design of preclinical & clinical research, consent issues, AE reporting • PUBLIC review of gene transfer protocols • 1989: First clinical gene transfer study (gene marking) - retroviral vector • 1990: First clinical gene transfer study (therapeutic intent) - retroviral vector
History, continued • 1995: No real clinical efficacy demonstrated, and NIH report concluded that enthusiasm had outstripped knowledge • Back to the bench for research on improved gene transfer methods • By 1995, NIH RAC • Had approved 149 GT clinical protocols • No dire consequences • Policy change: public review & approval only for GT protocols that presented novel or unresolved issues • 1997: Role of NIH RAC modified – still required public review, but not “approval” of novel GT protocols
History, continued 1999 • Jessie Gelsinger case – first human gene therapy death • All gene therapy trials placed on hold
History, continued 2000-2007 • X-linked SCID trials, using gamma retroviral vectors to deliver the corrective gene (IL2RG) to autologous hematopoietic progenitor cells • 5 of 20 pts developed T cell leukemia-like proliferative disorder, caused by INSERTIONAL ONCOGENESIS • Retroviral vector integrated adjacent to one or more cellular proto-oncogenes (LMO-2 in 4 of the cases), which increased their expression, leading to malignant transformation and outgrowth of clonal population of T cells
Gene Therapy Safety Issues • Observed to date • Insertional mutagenesis/oncogenesis • Immunogenicity – vector, transgene, FBS • Potential but not yet observed • Inadvertent transmission & expression in non-target cells (including germline, transplacental)
FDA guidances for gene therapy clinical trials • 2006 – Guidance on long-term follow up for delayed adverse events • 2006 – Supplemental guidance on testing for replication-competent retrovirus (RCR)
Summary • Regulatory and development approaches for HCT/Ps and gene therapies • Have evolved relatively recently, are still evolving • Acknowledge & address heterogeneity of products • There are few licensed HCT/Ps • There are no licensed gene therapies • Serious adverse events in early gene therapy trials prompted changes in preclinical & clinical requirements, and overall conduct of clinical trials