Download
1 / 4
40 likes | 426 Views
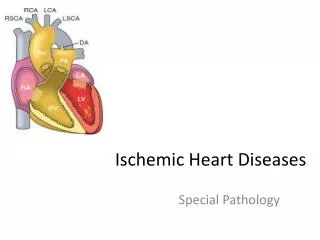
Cyanotic Heart Diseases TOF , TGA. Cyanosis occurs when approximately 5 g/100 mL of reduced hemoglobin is present in systemic blood By a lower reduced Hb-level The more is the Hb-level (Polycythemia)the more is the cyanosis The less is the Hb-level (Anemia) the less is the cyanosis

E N D
Cyanotic Heart DiseasesTOF, TGA Cyanosis occurs when approximately 5 g/100 mL of reduced hemoglobin is present in systemic blood By a lower reduced Hb-level The more is the Hb-level (Polycythemia)the more is the cyanosis The less is the Hb-level (Anemia) the less is the cyanosis • Tetralogy of Fallot is the most common cyanotic congenital heart defect, representing about 10% of all congenital heart defects. • Anatomically, there are four structural defects: • a large VSD • overriding of the aorta with respect to the • ventricular septum • subpulmonary stenosis causing right • ventricular outflow tract obstruction • right ventricular hypertrophy as a result. The pulmonary stenosis is central in the development of cyanosis And … The pulmonary stenosis murmur is the usual initial abnormal finding In addition, to these, a single S2 and right ventricular impulse at the left sternal border are typical findings. • Symptoms • The classical description of severe cyanosis, hypercyanotic spells and squatting on exercise developing in late infancy is now rare • hypercyanotic spells myocardial infarction, cerebrovascular accidents and even death if left untreated • hypercyanotic spells characterised by a rapid increase in cyanosis, usually associated with irritability or inconsolable crying because of severe hypoxia, and breathlessness and pallor because of tissue acidosis. • Signs • Clubbing • A single second heart sound • A loud harsh ejection systolic murmur • right ventricular outflow tract obstruction cyanosis will increase
Eisenmenger's syndrome with right-to-left shunting from pulmonary vascular disease following increased pulmonary blood flow and pulmonary hypertension Investigations: 1- ECG: right axis deviation and right ventricular hypertrophy. 2- The classic chest x-ray finding is a boot-shaped heart created by the small main pulmonary artery and upturned apex secondary to right ventricular hypertrophy 3- Echo Treatment of hypoxic spells: • O2 administration • knee-chest position (to increase venous return) • Sedation and pain relief (morphine is excellent) • Intravenous propranolol (or an alpha adrenoceptor agonist like phenylephrine), which probably works both as a peripheral vasoconstrictor and by relieving the subpulmonary muscular obstruction that is the cause of reduced pulmonary blood flow • Intravenous volume administration • Bicarbonate to correct acidosis • Muscle paralysis and artificial ventilation in order to reduce metabolic oxygen demand. When hypoxic spells occur, they are usually progressive. During a typical spell restlessness and agitation and crying inconsolably, squatting. Hyperpnea occurs with gradually increasing cyanosis In severe spells, prolonged unconsciousness and convulsions, hemiparesis, or death may occur. Independent of hypoxic spells, patients with tetralogy are at increased risk for cerebral thromboembolism and cerebral abscesses resulting in part from their right-to-left intracardiac shunt. Complete surgical repair Occasionally, palliative shunt surgery (Blalock-Taussig) between the subclavian artery and pulmonary artery is performed for complex forms of tetralogy of Fallot with more complete repair at a later time. Subacute bacterial endocarditis prophylaxis is indicated.
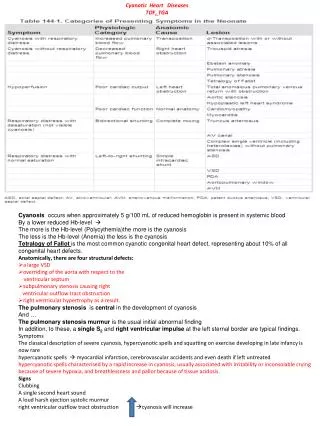
Clinical Manifestations: cyanosis is always present. It may be profound and life-threatening Quiet tachypnea and a single S2 When large VSD (mixing) CHF (Single SII, loud VSD murmer) Investigations: Typical “ECG” findings right axis deviation and right ventricular hypertrophy Chest x-ray: increased pulmonary vascularity, and the cardiac shadow is classically an egg on a string (egg-on-side) created by the narrow superior mediastinum TRANSPOSITION OF THE GREAT ARTERIES Although dextroposed transposition of the great arteries represents only about 5% of congenital heart defects, it is the most common cyanotic lesion to present in the newborn period Mixing can occur at the atrial (patent foramen ovale/ASD), ventricular (VSD), or great vessel (PDA) level. Treatment: prostaglandin E1 to maintain ductal patency a balloon atrial septostomy Complete surgical repair is most often an arterial switch
Congestive Heart Failure CLINICAL MANIFESTATIONS : HISTORY: Infants: poor feeding, failure to thrive, tachypnea, and diaphoresis with feeding. Older children: shortness of breath, easy fatigability, and edema. PHYSICAL EXAMINATION: (findings depend on whether pulmonary venous congestion, systemic venous congestion, or both are present). Tachycardia, a gallop rhythm, and thready pulses may be present with either cause. If left-sided failure is predominant, tachypnea, orthopnea, wheezing, and pulmonary edema are seen. If right-sided failure is present, hepatomegaly, edema, and distended neck veins are present. Treatment of Heart Failure