Download
1 / 1
10 likes | 158 Views
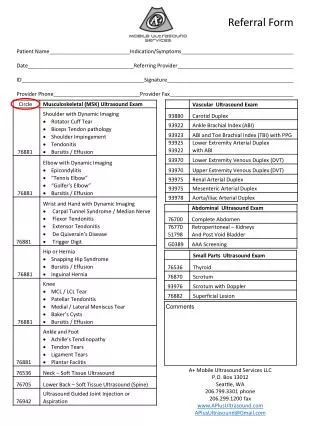
Referral Form Patient Name Indication/Symptoms Date Referring Provider ID Signature Provider Phone Provider Fax. Comments. A+ Mobile Ultrasound Services LLC P.O. Box 13012 Seattle, WA 206.799.3301 phone 206.299.1200 fax www.APlusUltrasound.com APlusUltrasound@Gmail.com.

E N D
Referral Form Patient NameIndication/Symptoms DateReferring Provider IDSignature Provider PhoneProvider Fax Comments A+ Mobile Ultrasound Services LLC P.O. Box 13012 Seattle, WA 206.799.3301 phone 206.299.1200 fax www.APlusUltrasound.com APlusUltrasound@Gmail.com