Download

1 / 82
950 likes | 2.28k Views
Diseases of Subcutaneous Fat. Endocrine Diseases. Ben Adams KCOM 5-11-05. Diseases of Subcutaneous Fat. Panniculitis May appear similar due to depth Two broad categories: Septal (classically E.N.) Lobular (Vascular). Erythema Nodosum. Acute Erythema Nodosum

E N D
Diseases of Subcutaneous Fat. Endocrine Diseases. Ben Adams KCOM 5-11-05
Diseases of Subcutaneous Fat • Panniculitis • May appear similar due to depth • Two broad categories: • Septal (classically E.N.) • Lobular (Vascular)
Erythema Nodosum Acute Erythema Nodosum • Crops of bilateral, deep, tender, 1-10 cm diameter, red nodules, on pretibial area (or other). • Lesions resolve over several days or weeks, leaving a bruise like area. (erythema contusiforme) which resolves without scarring. • Fever, malaise, leg edema, arthritis and other systemic symptoms may be present • Associated states (reactive process) • W>>M, TB, Streptococcal inf., Mycoplasma, Coccidioidomycosis, Yersinia, Salmonella, deep fungal infections, Sarcoidosis, drug (oral contraceptives). Pregnancy. Many others. • Idiopathic 35-55% of cases
Findings suggestive of a systemic cause for Erythema Nodosum • Synovitis • Diarrhea • Abnormal chest X-ray • Preceding upper respiratory tract infection • Elevated anti-Dnase B • Positive tuberculin skin test
Erythema Nodosum Chronic Erythema Nodosum • Distinguishing features: • Older women • Unilateral, Single lesion which spreads centrifugally to form annular plaques. Sometimes bilateral. • No systemic symptoms ( Possibly arthralgia ) • Less tender • No underlying disease • Prolonged course of months / years. • Key to diagnosis: Pretibial, no systemic complaints. Biopsy seldom required. • DDX: erythema induratum (post. Calf), syphilitic gummas (unilateral). Subcutaneous fat necrosis assoc with pancreatits etc. – systemic.
Erythema Nodosum • Histologic Features • Septal infiltrate of neutrophils (early), other mononuclear cells. Histiocytes and Multinucleated Giant cells may predominate older lesions. Some foamy histiocytes may be seen. • Meischer’s radial granulomas: Aggregates of histiocytes around stellate clefts is characteristic not diagnostic.
Erythema Nodosum Septa are widened and edematous, and infiltrated by lymphocytes and neutrophils
Miescher's microgranulomas within septa. Erythema Nodosum
Erythema Nodosum • Treatment: • Treat underlying causes. • NSAIDS, bed rest / reduced activity • Potassium Iodide: Increase to control. • Watch for hypothyroidism. • Reports of EN triggered by SSKI • Intralesional / systemic Steroids • Refractory cases: anti-malarials, colchicine. • Most cases resolve in 3-6 wks.
Nodular Vasculitis • AKA: Erythema Induratum • Tender subcutaneous nodules of calves of middle aged, thick – legged women. Bilateral, often ulcerate and recur over years. • Pathology: Arteritis, venulitis of septal vessels with substantial necrosis of lobular adipocytes resulting in suppuration and perforation. Granulomatous inflammation. • DDX: Erythema induratum. TB testing, PCR of affected tissue for mycobacterium. • Treatment: SSKI (50% effective). Other agents used in E.N.
Nodular Vasculitis • Nodular lesions on the lower leg with evidence of ulceration
Sclerosing Panniculitis(Lipodermatosclerosis) • Presentation: Development of woody induration of lower calves (esp. left) with appearance of inverted champagne bottle. Induration begins near ankles and slowly progresses proximally. Most common W > 40 years. May be painful. • Pathogenesis: venous insufficiency with hypoxia of center of fat lobule. May not be apparent venous disease. • Histopathology: Necrosis of fat lobules with ghost cells (pale cells no nuclei). Foamy histiocytes, inflammatory cells and septal thickening with fat microcyst. • Biopsy should be avoided. Heals poorly. Venous eval. • TX - Treat venous insufficiency. • Compression stockings (may be painful). • Stanozolol decreases perivascular fibrin, decreases pain in 3 wks and induration in 8 wks.
Lipomembranous change, consisting of cystic formation with elaborate papillary configurations Sclerosing Panniculitis
Physical Panniculitis Sclerema Neonatorium • Presentation: Gravely ill, premature neonate’s skin begins to harden on buttocks and LE and rapidly spreads to involve entire body except palms, soles and genitalia. • Mobility affected by induration. • Rapidly fatal. • Child is very ill. • Histopathology: Enlarged adipocytes filled with needle like clefts in radial array. • TX: treat underlying disease.
Needle-shaped clefts within lipocytes, in the absence of inflammation. Sclerema Neonatorium
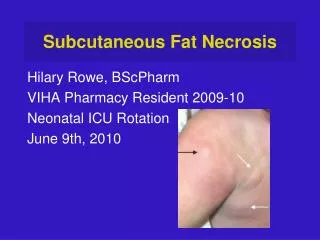
Subcutaneous Fat Necrosis of the Newborn. • Presentation: Asymptomatic, firm, rubbery nodules on upper back, buttocks, cheeks and proximal extremities. May fuse into plaques which resolve over several months without scarring. • Occurs during first 4 weeks of life. • Child is otherwise healthy • Associated with perinatal hypothermia, asphyxia and difficult labor and maternal drug use. • Rarely, hypercalcemia occurs during the episode. • Histopathology: Lobular panniculitis with radial needle clefts in adipocytes. • Fine needle aspiration has been used to DX.
Indurated plaques on the trunk Subcutaneous Fat Necrosis of the Newborn.
Needle-shaped clefts in radial configuration are present within giant cells. Subcutaneous Fat Necrosis of the Newborn.
Synonyms: Popsicle / equestrian panniculitis. Presentation: Within several days of cold exposure, affected skin becomes mildly erythematous with nontender firm Sub-Q nodules. Face, thighs and scrotum. Typical patients: (Hx of cold exposure). Infants and young children. Black > Whites. Scrotal disease: prepubertal, 9-14 yr old male who is over weight. Bilateral, painful, no transillumination. Resolves in several days to weeks without TX. Cold Panniculitis
Erythematous, violaceous plaques on the thighs in a case of equestrian cold panniculitis. Cold Panniculitis
Post Steroid Panniculits • Firm sub-Q nodules form within one month of rapid withdraw from high dose systemic steroids. • Predominantly children. • Most cases resolve. May have to restart steroids and wean more slowly. Traumatic Panniculitis • Trauma, often not recalled, induces a firm mildly tender lipoma like sub-Q mass. • Heals with fibrosis of septa.
Factitial Panniculitis • Factitial injection of foreign substances into the skin. Medical personal are common patients. • DX: • Careful HX. Fits no other pattern. • Healing injection site, biopsy revealing foreign material, polarized light micro, Mass spectroscopy in difficult cases is suspicion is high.
Sclerosing Lipogranuloma • Granulomatous and fibrotic reaction from intentional, often cosmetic, injection of mineral oils, silicon or guayacol (Mexico). • Presentation: Up to ten years after implantation, skin becomes erythematous, hyperpigmented and indurated with a lumpy quality of sub-q. Due to migration of material, features may extend beyond the implantation site. • 66% autoimmune finding (+) ANA, Raynauds, Sjogrens ect. 10% connective tissue disease usually scleroderma. • Histologically: Swiss cheese appearance of panniculus. Histiocytes with ingested material. Fibrosis.
Sclerosing Lipogranuloma 2nd to Cosmetic Paraffin injections
Oil granuloma. Numerous vacuolated spaces, in this case due to grease gun injury. Sclerosing Lipogranuloma
Pancreatic Panniculitis • Fat necrosis 2nd to Pancreatitis or pancreatic carcinoma. May be first sign of malignancy (40%). Digestive enzymes cause damage. • Presentation: Tender or painless, erythematous Sub-q nodules 1-5 cm. In diameter. Lower leg is affected 90%. Lesions typically number <10 (may be 100s). Involutes with scarring. • Assoc findings: abd pain (sometimes), arthritis (FFA in synovial fluid), pulm. infiltrates. • DX: pancreatic workup amylase, lipase. • Peripheral eosinophila in Pancreatic CA. • Histology: fat necrosis, Ghost cells. Finely stippled Basophilic material (Calcium) with rim of necrotic cells. Inflammatory infiltrate at periphery.
Neutrophilic inflammation, cellular necrosis, and deposition of homogeneous basophilic material due to saponification of fat by calcium salts. Pancreatic Panniculitis
Alpha-1 Antitrypsin Deficiency Panniculitis • 1:2500 of European decent have homozygous deficiency of enzyme which inhibits neutrophil elastase. The genetic defect results in a molecule that cannot be released from its production sites in hepatocytes. • AAT is 1 of the 3 most common lethal genetic diseases among whites. • Presentation: After minor trauma, painful nodules appear on extremities and trunk. Lesions may form draining sinuses. • M=F, 20-40 years. • Histopathlogy: Dissolution of septae. Islands of normal fat floating in spaces of destroyed septae.
Purpuric nodules on the ankle Alpha-1 Antitrypsin Deficiency Panniculitis
Alpha-1 Antitrypsin Deficiency Panniculitis • DX • Constellation of Liver dysfunction and Pulmonary dysfunction with skin lesions • Serum AAT levels • AAT function analysis • TX • Replace enzyme (prolastin) • Dapsone, doxycycline
Cytophagic Histiocytic Panniculitis • Multi-system disease with widespread, painful sub-q nodules which may break down and form ulcerations. • Progressive febrile illness with heptomegaly, pancytopenia, HTG. • Etiology: Proliferation of histiocytes. Triggered by viral infection or 2nd to lymphomas. • Benign: (-) EBV • Malignant (+) EBV, B or T cell Lymphoma. • HIV assoc. • Histopathology: Infiltration of fat lobules with histiocytes with fat necrosis. Bean bag cell stuffed with RBC. • Clonal B or T cell proliferation = malignant. • TX: Benign - cyclosporine induces permanent remissions. Malignant - Chemo or bone marrow.
Cytophagic Histiocytic Panniculitis Subcutaneous nodules with purpura
Macrophages engaged in cytophagic activity. Some of them have the appearance of ‘bean bag cells’ Cytophagic Histiocytic Panniculitis
Misc. Panniculitis • Eosinophilic Panniculitis • Prominent infiltration with eosinophils assoc with arthropod bites, parasites, contact derm, Well’s, bacteria, injections. • Gouty Panniculitis • Uric acid in Sub-Q leading to fat necrosis.
Lipoatrophies • Total • Partial • Centrifugal • Semicircular • Lipoatrophia Annularis • Localized • HIV associated
Total Lipodystrophy 2 types: Congenital vs Acquired. Both are assoc. with D.M. (lipoatrophic diabetes) 1.) Beradinelli - Seip (congenital) • Autosomal recessive. Hypermetabolic state. • General: Paucity of fat at birth with voracious appetite, increased height velocity, muscular hypertrophy, genital enlargement, mild MR, protuberant abdomen, HTG. Hypertrophic cardiomyopathy, pul stenosis. DM resistant to therapy. • Cutaneous: AN (often generalized), Hypertrichosis with abundant curly scalp hair. • Death in young adulthood from DM, cardiac, liver dx. • TX: fenfluramine reduces hypermetabolic state.
Congenital Total Lipodystrophy AN and Loss of Bichat’s fat pad
Total Lipodystrophy 2.)Seip - Lawrence (acquired) • Begins <15 yrs old, often <5yrs (not at birth) • Well defined illness precedes 30 % of cases. • Presentation: As in congenital, but less striking. AN with DM is common. Severe liver involvement is more common (death). Loss of fat may begin local and generalize or start generalized. • TX: etretinate has helped AN in some.
Partial Lipodystrophy (Inherited Forms) Kobberling-Dunnigan syndrome • Autosomal dominate. • At puberty adipose tissue is lost from extremities, gluteal and truncal areas with fat accumulation on the neck and face. • DM with AN, HTG, hirsutism, PCOS after age of 20 years. Other inherited forms: • Onset early infancy with adipose tissue loss localized to the face and buttocks. Rieger anomaly: tooth and eye abnormalities: hypoplasia of the iris and iris strands to the peripheral cornea. • Bone age and dentition are retarded. • DM late. No AN.
Partial Lipodystrophy (Acquired Forms) Progressive Partial Lipo. (Barraquer-Simons) • W > M, Present first or second decade. • After a febrile illness, diffuse and progressive loss of fat beginning on face and scalp and progressing downward to iliac crest. Sparing of LE. • No discomfort or inflammation. • Low C3 levels are assoc. and proteinuria occurs in in 50% of these cases. • 3rd trimester intrauterine death may occur.
Progressive Partial Lipo. Loss of buccal fat and AN.
Lipoatrophies • Centrifugal • One type is seen primarily in infants from Japan. 90 % are under 5 years. • Centrifugally spreading loss of abdominal fat over 3- 8 years with regional lymphadenopathy. • Resolves completely after progression stops. • Semicircular • Adult women affected with single or multiple, asymptomatic, symmetric depressions of anterolateral thigh. • Often after trauma. Resolves in several years. • Annular Atrophic panniculitis • 10cm band of atrophy, bilaterally, around the ankles of children and young adults. Rare.
Lipoatrophies Lipoatrophia Annularis • Bracelet like constrictions of upper extremities 1-2 cm wide on women following a period of swelling and erythema of extremity. • Arthralgias and Pain of affected extremity • Persist up to 20 years. Localized lipodystrophy • 2nd to injection of medications esp. insulin. HIV assoc. Lipodystrophy. • Occurs in effectively Treated Aids Patients with reverse transcriptase inhibitors and protease inhibitors. • Fat redistribution from face, buccal, buttocks and limbs is lost to neck , upper back and inter abdominal areas.
Localized lipodystrophy Insulin injection lipodystrophy