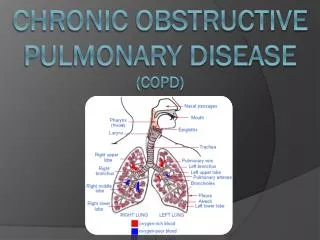
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
360 likes | 679 Views
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD). ABHAY DESHMUKH, MD June 14, 2012. OBJECTIVES. TO DEFINE COPD AND ITS STAGING TO DISCUSS THE PATHOGENESIS TO UNDERSTAND THE MANAGEMENT PRINCIPLES. PROBLEM OF COPD. It is the third leading cause of death in the United States

CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
E N D
Presentation Transcript
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) ABHAY DESHMUKH, MD June 14, 2012
OBJECTIVES • TO DEFINE COPD AND ITS STAGING • TO DISCUSS THE PATHOGENESIS • TO UNDERSTAND THE MANAGEMENT PRINCIPLES
PROBLEM OF COPD • It is the third leading cause of death in the United States • COPD should be viewed as a systemic disease with important pulmonary and extra-pulmonary manifestations • Dr Nicholas Gross once compared it to defining love, “everybody knows what it is, but each individual describes it differently.” Morbidity and mortality: 2009 chart book on cardiovascular, lung, and blood diseases. National Heart, Lung, and Blood InstituteBethesda (MD)2009
DEFINITION OF COPD • Chronic obstructive pulmonary disease (COPD) is a preventable and treatable disease with some significant extra-pulmonary effects that may contribute to the severity in individual patients. Its pulmonary component is characterized by airflow limitation that is not fully reversible. The airflow limitation is usually progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for Diagnosis, Management and Prevention of COPD. GOLD; 2010
DIAGNOSIS OF COPD • COPD is confirmed when a patient, who has symptoms that are compatible with COPD, is found to have airflow obstruction (FEV1/FVC ratio less than 0.70 and an FEV1 less than 80 percent of predicted) and there is no alternative explanation for the symptoms and airflow obstruction (eg, bronchiectasis, vocal cord paralysis, tracheal stenosis) Mohamed Hoesein F.A., Zanen P., Lammers J.W.: Lower limit of normal or FEV1/FVC < 0.70 in diagnosing COPD: an evidence-based review. Respir Med 105. (6): 907-915. 2011
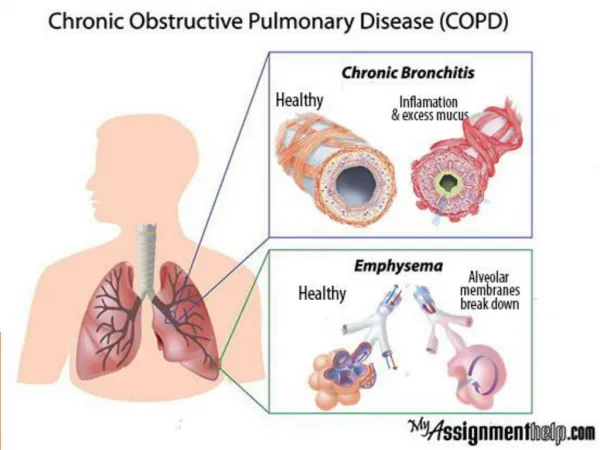
Chronic bronchitis is defined by a chronic productive cough for three months in each of two successive years in a patient in whom other causes of chronic cough have been excluded. • Emphysema is defined by abnormal and permanent enlargement of the airspaces that are distal to the terminal bronchioles. This is accompanied by destruction of the airspace walls, without obvious fibrosis.
Asthma is "a chronic inflammatory disorder of the airways in which many cells and cellular elements play a role. The chronic inflammation is associated with airway responsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness and coughing, particularly at night or in the early morning. These episodes are usually associated with widespread, but variably, airflow obstruction within the lung that is often reversible either spontaneously or with treatment"
RISK FACTORS • Cigarette smoke, containing more than 6000 molecules and 10 free radicals per puff, can initiate an inflammatory response in many ways • Tobacco smoke remains the most recognized cause for COPD globally • There are other exposures that can cause COPD related to occupation (various organic and inorganic dusts, chemical fumes, smoke), air pollution and biomass fuels • Cannabis smoke may contribute to COPD • Given that only 20% to 30% of individuals who smoke appear to develop evidence of COPD, it seems clear that there are likely COPD susceptibility genes and probably genes that might influence severity and response to various medications
GENES FOR COPD • Alfa1-Antitrypsin deficiency- SERPINA1 • Susceptibility genes for developing COPD or lower lung function- EPHX1, GST, MMP12, TGFB1, SERPINE2 • Nicotine dependence and lung cancer- CHRNA3/5 Nakamura H.: Genetics of COPD. Allergol Int 60. (3): 253-258.2011
SMOKING CESSATION • Nicotine chewing gum or patch (NRT) has shown to increase smoking cessation rates by approximately 1.5- to 2-fold after 12 months. • Bupropion inhibits the neuronal uptake of noradrenaline and dopamine. Give 150 mg qday x 3 days, then 150 mg BID for 7-12 weeks, start treatment 1 week before quit date. • Varenicline is a partial agonist at nicotinic ɑ4 β2 receptors. Give 0.5 mg qday x 3 days, then 0.5 mg BID for 4 days, then 1 mg BID for up to 12 weeks. • Counseling has been shown to augment the effects of pharmacologic intervention Cahill K., Stead L.F., Lancaster T.: Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev 2. 2011
PULMONARY REHABILITATION • Pulmonary rehabilitation is an important nonpharmacologic therapeutic in COPD, yet it remains underutilized. • Typical components include patient assessment, exercise training, education, nutritional intervention, and psychosocial support. • Has positive impacts on health-related quality of life, reduced symptoms, improved peripheral muscle strength, exercise endurance, reduced number of hospital days, and improved psychosocial status, reduction in hospitalizations and emergency room visits Pulmonary rehabilitation: joint ACCP/AACVPR evidence-based clinical practice guidelines. Chest 131. (Suppl 5): 4S-42S.2007
OXYGEN THERAPY • Oxygen therapy is well established to increase survival and is indicated for patients with an arterial oxygen tension (PaO2) of less than 55 mm Hg. • Goal is to maintain saturations greater than 90% during rest, sleep, and exertion. Anthonisen N.R.: Long-term oxygen therapy. Ann Intern Med 99. (4): 519-527.1983
PHARMACOLOGIC MANAGEMENT • Given that airflow obstruction is the primary concern in COPD, it follows that short-acting and long-acting bronchodilators form the cornerstone of pharmacologic management. • Inhaled short-acting β2 agonists such as albuterol have a more rapid onset of effect and shorter duration of action than short-acting anticholinergic agents such as ipratropium and thus are more often prescribed as “rescue” medications to relieve acute bronchospasm.
Patients that have persistent symptoms and require daily use of short-acting agents are recommended to switch to long-acting (12 hours) bronchodilators such as salmeterol and the long-acting antimuscurinic agent (LAMA), tiotropium (24 hours). • Several studies have identified the long-acting β2 agonists (LABAs) to be effective in reducing symptoms, and improving lung function and health-related quality of life in patients with COPD. Optimizing treatment of chronic obstructive pulmonary disease: an assessment of current therapies. Am J Med 120. (8 Suppl 1): S4-S13. 2007
Given the importance of inflammation in the pathogenesis of COPD, inhaled corticosteroids (ICS) are typically the next line of therapy recommended for patients. • ICS should be added to bronchodilators and should not be used as monotherapy in COPD. • ICS given to patients with stable COPD for longer than 6 months led to about 30% reduction in the total number of exacerbations. The effects of inhaled corticosteroids in chronic obstructive pulmonary disease: a systematic review of randomized placebo-controlled trials. Am J Med 113. (1): 59-65.2002
For patients not optimally controlled in terms of symptoms with frequent use of rescue inhalers and with evidence of frequent exacerbations, combination therapy with ICS and either LABAs or LAMAs are recommended. • In a study of 782 patients with COPD, fluticasone propionate/salmeterol 250/50 μg significantly reduced the annual rate of moderate to severe exacerbations by 30.5% compared with salmeterol alone (P<.001) • The most common side effects seen with ICS include skin bruising, oropharyngealcandidiasis, and voice alterations. Effect of fluticasone propionate/salmeterol (250/50 microg) or salmeterol (50 microg) on COPD exacerbations. Respir Med 102. (8): 1099-1108.2008
Triple therapy comprising fluticasone/salmeterol/tiotropium in those with very advanced disease was superior to the use of the fluticasone/salmeterol or tiotropium/salmeterol in terms of improvements in symptoms and reduced rescue medication requirements • Due to its narrow therapeutic index and potential side effects, theophylline has been relegated to a third-tier option for COPD Gaebel K., McIvor R.A., Xie F., et al: Triple therapy for the management of COPD: a review. COPD 8. (3): 206-243. 2011
Diagnostic Evaluation of Patients with Suspected COPD Exacerbation Perform routinely Pulse oximetry: Hypoxemia Perform if hospitalized Arterial blood gas: Hypercarbia, Hypoxemia Chest radiography: Alternate sources of dyspnea Complete blood count: Anemia, Leukocytosis, Polycythemia Electrocardiography: Cardiac arrhythmias, Cardiac ischemia Metabolic panel: Electrolyte disturbances, Hypo- or hyperglycemia Metabolic acid-base changes Consider performing, especially if patient is not responding to conventional exacerbation treatment Brain natriuretic peptide: CHF (one third of dyspnea in chronic lung disease may be attributable to CHF), Cardiac enzyme measurement: Cardiac ischemia (myocardial infarction is underdiagnosed in patients with COPD)
MANAGEMENT OF ACUTE EXACERBATION • Acute exacerbations of COPD are associated with in-hospital mortality rates of about 10% • Nebulized formulations of rapidly acting bronchodilators should be used aggressively. • Supplemental oxygen should be given to maintain the PaO2 above 60 mm Hg and the SaO2 above 90% • Up to 50% to 80% of exacerbations may be associated with pathogens known to colonize the respiratory tract, including various viruses and Haemophilusinfluenzae, Streptococcus pneumoniae, and Moraxellacatarrhalis. • The more significant the symptoms of cough, sputum, and dyspnea and the more purulent the sputum, the more likely patients will benefit from empiric antibiotic therapy.
Empiric Antibiotics for COPD exacerbations • Amoxicillin/clavulanate: 875 mg orally twice daily for 5 days • Levofloxacin (Levaquin): 500 mg daily for 5 days • Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2006;(2):CD004403
ACUTE EXACERBATION CONTINUED… • Systemic glucocorticoids have been shown to reduce recovery time, reduce hospital time, reduce treatment failures, decrease risk of relapse and improve airflow limitation. Prednisone 30 to 60 mg/d for 7 to 10 days. There does not seem to be a difference between intravenous versus oral delivery in terms of outcomes. • Noninvasive positive-pressure ventilation has been shown to be able to negate the need for intubation and reduce mortality for severe exacerbations, and should be started early. Bakri F., Brauer A.L., Sethi S., et al: Systemic and mucosal antibody response to Moraxellacatarrhalis after exacerbations of chronic obstructive pulmonary disease. J Infect Dis 185. (5): 632-640. 2002
Macrolide antibiotics have both antimicrobial and anti-inflammatory effects. • Recently a prospective double-blind, placebo-controlled trial was conducted in which 1142 patients with a clinical diagnosis of COPD on supplemental oxygen and/or having exacerbations within the previous year were randomized to receive either azithromycin 250 mg or placebo daily for 1 year. There was significant reduction in time to first exacerbation (P<.0001), rate of acute exacerbations (P = .008), and quality-of-life scores (P<.006). Chronic azithromycin decreases the frequency of chronic obstructive pulmonary disease exacerbations. Am J RespirCrit Care Med 183. A6416. 2011
Lung volume reduction surgery versus lung transplantation • Patients with FEV1 less than 20% predicted, and either diffusing capacity for carbon monoxide less than 20% predicted or homogeneous pattern of emphysema on computed tomography, are at high risk for death • In a carefully selected subgroup of individuals with low exercise tolerance post rehabilitation and upper lobe–predominant emphysema, LVRS offers substantial survival, functional, physiologic, and quality-of-life benefits • Lung transplantation can be considered in patients who do not meet criteria for LVRS but who are otherwise good candidates Lung transplantation and lung volume reduction surgery versus transplantation in chronic obstructive pulmonary disease. Proc Am Thorac Soc 5. (4): 447-453.2008
Key recommendations for practice • Noninvasive positive pressure ventilation improves respiratory acidosis and decreases respiratory rate, breathlessness, need for intubation, mortality, and length of hospital stay. A • Inhaled bronchodilators (beta agonists, with or without anticholinergics) relieve dyspnea and improve exercise tolerance in patients with COPD. A • Short courses of systemic corticosteroids in patients with COPD increase the time to subsequent exacerbation, decrease the rate of treatment failure, shorten hospital stays, and improve FEV1 and hypoxemia. A
Antibiotics should be used in patients with moderate or severe COPD exacerbations, especially if there is increased sputum purulence or the need for hospitalization. B • Smoking cessation reduces mortality and future exacerbations in patients with COPD. A • Long-term oxygen therapy decreases the risk of hospitalization and shortens hospital stays in severely ill patients with COPD. B
References • Chronic Obstructive Pulmonary Disease: A Concise Review. Medical Clinics of North America- Volume 95, Issue 6 (November 2011). • UpToDate 2012. • Harrison’s Principles of Internal Medicine, 18th edition 2012. • Management of COPD exacerbations. AFP March 1, 2010 Volume 81, Number 5.