Download
1 / 52
530 likes | 822 Views
Demonstrate an understanding of main connections and functions of the basal ganglia. TE 4.2. Basal ganglia. The basal ganglia are paired groups of forebrain nuclei found deep within the cerebral hemispheres that help to control movement.

E N D
Demonstrate an understanding of main connections and functions of the basal ganglia TE 4.2
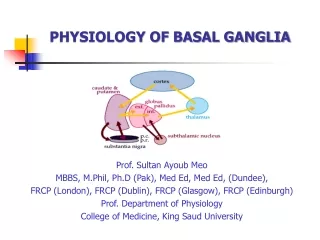
Basal ganglia • The basal ganglia are paired groups of forebrain nuclei found deep within the cerebral hemispheres that help to control movement PM4 TE 4.2
http://cti.itc.virginia.edu/~psyc220/kalat/JK246.fig8.15.basal_ganglia.jpghttp://cti.itc.virginia.edu/~psyc220/kalat/JK246.fig8.15.basal_ganglia.jpg
http://www.swmed.edu/stars/images/neurodisslides/Slide18.JPG Sagittal section
http://www.swmed.edu/stars/images/neurodisslides/Slide18.JPG
Coronal section http://www.stanford.edu/group/hopes/basics/braintut/f_ab18bslgang.gif
Connections in the basal ganglia http://thalamus.wustl.edu/course/cerebell.html
The overall function of this loop (direct pathway) is to select a particular movement or a sequence of movements while suppressing others PM4 TE 4.2
Globus pallidus and Substantia nigra inhibit the thalamus (-) • Striatum inhibits globus pallidus, which in turn releases thalamus from inhibition (-) • The Thalamus through its projections to cerebral cortex release the selective movements (+) PM4 TE 4.2
Basal ganglia is often described in terms of a "brake hypothesis". • Fine balance must be maintained between suppression of all movements and the release of appropriate movements. • The correct balance is maintained by the Substantia Nigra pars Compacta (+). • It provides excitatory D1 Dopamine input to the Putamen PM4 TE 4.2
Direct pathway PM4 TE 4.2
PD • Difficulty in initiating movements because of reduced dopaminergic input from substantia nigra pars compacta • Under activity in direct pathway causes too much inhibition of thalamus and prevents initiation of movements PM4 TE 4.2
Parkinson’s Disease • A progressive, primary neuro degenerative disorder • Affects Substantia Nigra and Corpus Striatum (Caudate Nucleus and Putamen) PM4 TE 4.2
Aetiology / Epidemiology • Cause unknown • No known social, economic or geographical variations • M=F • Prevalence -100-180 per 100,000 population • Incidence – 4-20 per 100,000 • 1 per 100 over 75 yrs of age • Average onset – 60 yrs • 1 in 7 diagnosed < 50yrs PM4 TE 4.2
Pathophysiology Substantia Nigra (Dopamine producing nuclei) • Death of cells • Loss of Dopamine production • Lack of inhibition of cholinergic neurons • Unopposed Excitation • Normal balance of excitation and inhibition lost • Smooth movement / Lack of movement control • Lack of inhibition of reticular spinal + vestibulospinal tracts • Excessive contraction of postural muscles PM4 TE 4.2
Pathophysiology • The amount of dopamine in the basal ganglia decreases by about 13% per decade after age 20 • consequently motor activity becomes less well controlled with advancing age • As substantia nigra dopamine cells die their synapses in the basal ganglia disappear • 60% of nigral neurons and 80% of striatum dopamine must be lost before symptoms are seen PM4 TE 4.2
The deficits tend to fall into one of two categories: • the presence of extraneous unwanted movements • or an absence or difficulty with intended movements. PM4 TE 4.2
Tremor • Head rotation • Jaw opening n closing • Tongue in n out • Pill-rolling • 5-6 Hz frequency • Present at rest, absent in sleep, increased by emotion, excitement or fatigue and on being watched • Cause: damage to inhibitory nigro-striatal pathways - excessive excitatory output from the striatum – facilitation of oscillatory bursts of activity in thalamic neurons – excitation of localised areas of cerebral cortex PM4 TE 4.2
Rigidity • Uniform increase in tone in all muscle groups of the area involved • Resistance throughout the whole range of passive movement • Lead-pipe: smooth rigidity • Cog-wheel: muscles yield in a seiries of jerks • Rigidity decreases on support and relaxation • Increases by mental concentration and active movements of other parts of the body • More in neck and forearm muscles • Exaggerated postural fixation • Decreased by surgical incision in globus pallidus and by administration of L-dopa PM4 TE 4.2
Bradykinesia, hypokinesia • Slowness and poverty of movement • Voluntary and automatic movements are slow, reduced in amplitude and range • Loss of arm swing during walking • Micrographia • Latent period between stimulus and response • Fine movements are more affected PM4 TE 4.2
Difficulty in modifying range and speed • Inability to maintain repetitive movements or perform rapidly alternating movements (Dysdiadochokinesia) • Lack of rotation component • Tends to sit still • Mask face PM4 TE 4.2
Reduced thoracic expansion • Lead to respiratory complications • Mastication and swallowing affected • Speech-slurred, monotonus • Constipation PM4 TE 4.2
Flexed posture • Rounded shoulders, head held forwards, Scoliosis • Loss of normal trunk rotation as normal balanced activity between the flexors and extensors is lost • Lack of rotation leads to lack of arm swing • the characteristic shuffling gait • Posture can be voluntarily corrected but only temporarily • lean far forward, chase their CG to avoid falling over - anteropulsion or festination PM4 TE 4.2
Defective postural reflexes • Anti-gravity mechanisms –good • Postural fixation, protective reactions, righting reflexes, tilting reactions, locomotive reactions – affected • Typical flexed posture • Sticks to the position • Can easily fall • Rotations, transitions is affected • Weight shift is affected –shuffle • Festinant gait – rapid short steps forward • Retropulsion, propulsion PM4 TE 4.2
Stretch reflexes • Reduced in amplitude • Plantar reflex - flexor PM4 TE 4.2
Poor balance Postural mechanisms Rigidity Hypokinesia MUSCULOSKELETAL SYSTEM Flexed posture Contracture (Fixed kyphosis and loss of pelvic mobility) Faulty balance PM4 TE 4.2
Autonomic disturbances • Urinary dysfunction • Weight loss • Dysphagia • Constipation • Orthostatic hypotension • Excessive sweating • Excessive salivation • Flushing of the skin • Sensation of heat • Tolerate cold better than heat PM4 TE 4.2
Pain and aching • Sleep disturbance • Psychiatric problems • Depression • Dementia • Disability and handicap • Impaired quality of life • Family and carers affected indirectly PM4 TE 4.2
Altering mechanisms Bradykinesia Rigidity MUSCULOSKELETAL CARDIOPULMONARY SYSTEM de-conditioning COMPOSITE EFFECT Bradykinesia Physical Slow and ineffective function EMOTIONAL Depression SOCIAL withdrawal PM4 TE 4.2
Social problems • Drool while eating • Difficulty with voice production • Lack of facial expression • Impaired mobility • Social isolation • Depression PM4 TE 4.2
Parkinsonism • Drug induced • Multiple infarction • Degenerative conditions • Progressive supranuclear palsy (PSP) • Multiple system atrophy (MSA) PM4 TE 4.2
Diagnosis • No diagnostic test • Primarily clinical • Based on history -slow onset • clinical examination • early symptoms include clumsiness, tremor and movement difficulties often on one side of the body • Depression and dementia often develop • Rate of progression varies PM4 TE 4.2
Scales for progression and disability • Hoen and Yahr stage of disease • the interrelationship of balance disturbance and disability • New York University disability scale • Rates rigidity, trmor, bradykinesia, gait and postural stability • Northwestern University disability scale • Activities of daily living PM4 TE 4.2
Hoen and Yahr stage of disease • Stage 1 • Unilateral involvement with minimal or no functional involvement • Stage 2 • Bilateral or midline involvement without balance impairment • Stage 3 • Impaired righting reflexes (balance) with some restriction in functional activity but with capacity for living independent lives • Stage 4 • Severely incapacitating disease but are still able to walk and stand without assistance • Stage 5 • Confined to bed and a wheel chair except when assisted PM4 TE 4.2
Aims of management • No cure • Goals • Improve function / safety • Delay loss of independence • Medical management – Drugs / Surgery • Therapeutic management – MDT approach PM4 TE 4.2
Young patient emphasis on long term considerations • Older patient focus is on symptomatic benefit in the near term with as few adverse effects as possible PM4 TE 4.2
Medical management • To provide control of signs and symptoms for as long as possible while minimizing adverse effects • Medications usually provide good symptom management for 4-6 years, after this disability progresses despite medical management • Patients develop long term motor complications including fluctuations and dyskinesia • As PD progresses fewer dopamine neurones are available to store and release the derived dopamine so the patients clinical state begins to fluctuate more PM4 TE 4.2
Drug Treatment • Levodopa (L-dopa) or Dopamine receptor agonists • L-dopa is converted to dopamine in the brain • L-dopa is given with a decarboxylase inhibitor (carbidopa) otherwise 90% would be converted to dopamine in the body causing side effects • dopamine agonists stimulate dopamine receptors • Selegiline (Deprenyl) • inhibits monoamine oxidase (MAO-B) and reduces dopamine breakdown • Benzatropine (atropine was used before L-dopa) • inhibits acetylcholine receptors PM4 TE 4.2
Initial pharmacotherapy in early PD Nice guideline PM4 TE 4.2
Tremor specific drugs can be used if that is the main cause of disability • Stereotactic surgery or thalamotmy (destructive surgical procedures on the thalamus) • One technique is pallidotomy which targets the globus pallidus which can give good results for patients with severe tremor or involuntary movement. PM4 TE 4.2
Dystonic movements as a side effect of pharmacologic agents • May interfere with function PM4 TE 4.2
Physiotherapy Management • Early - Prevention / Education • Middle - Compensation strategies • Late - Respiratory status - Function - Aid and adaptations - Palliative care PM4 TE 4.2
Treatment Approaches Eclectic Approach • Normal movement re-education • Biomechanical approach • Relearning motor sequences • Mental rehearsal • Cueing strategies • General physiotherapy modalities • Exercise – esp rotation • Functional re-education • Balance re-education PM4 TE 4.2
Principles of Treatment • Assessment to identify treatment priorities & identify goals • Early implementation of a preventative exercise programme • Targeted intervention focusing on areas of deterioration • Use of structured programmes based on the principles of psychometric learning to address motor deficits PM4 TE 4.2
Physiotherapy • Gait reeducation, improvement of balance and flexibility • Enhancement of aerobic capacity • Improvement of movement inititation • Improvement of functional independence, including mobility and ADL • Provision of advice regarding safety in the home environment PM4 TE 4.2
Compensation strategies • Breakdown complex movement sequences into simple component parts • Arrange parts in a logical, sequential order • Utilise prior mental rehearsal of the whole movement sequence • Perform each part separately, ideally ending in a stable resting position from which next step can be initiated • Execute each part under conscious control • Avoid simultaneous motor or cognitive tasks • Use appropriate visual, auditory and somatosensory cues to ninitate and maintain movement PM4 TE 4.2
Cues • Visual (spatial) practice walking -stripes on floor Steeping over lines • Auditory (Rhythm) listening to beats to initiate movement or maintain cadence • Auditory/visual (spatial) verbal prompt/ to a visual cue to negotiate on steps • Somatosensory (rhythm) steeping back to start walking rocking side to side • Mental rehearsal (spatial) visualisation of walking Memorising parts of sequence PM4 TE 4.2
Occupational therapy • Speech and language therapy • Palliative care PM4 TE 4.2
Life style adjustments that affect both physical nature of the condition and patients attitude to having PD PM4 TE 4.2