Cardiovascular Consequences of COX-2 Inhibition: A Comprehensive Overview
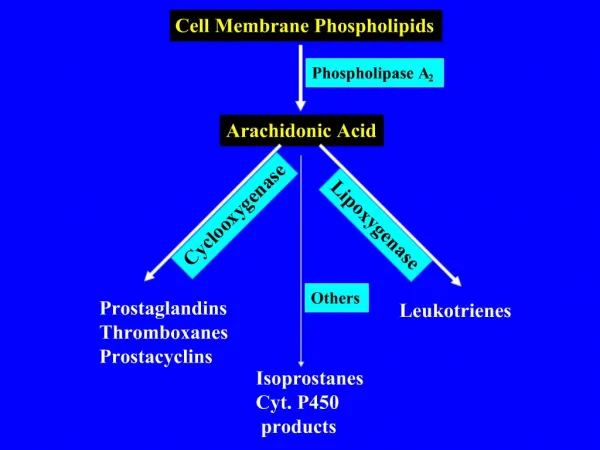
The study investigates the biological underpinnings of COX-2 inhibition and its cardiovascular ramifications. COX-2 selective inhibitors, while effective in reducing inflammation, are shown to affect prostacyclin biosynthesis significantly. A large portion of prostacyclin production is COX-2 dependent, which plays a critical role in modulating thrombotic responses. The differential selectivity of COX-2 inhibitors can increase the risk of thrombotic events in predisposed individuals. This review highlights the physiological impact of COX isoforms on thrombosis and vascular health.

Cardiovascular Consequences of COX-2 Inhibition: A Comprehensive Overview
E N D
Presentation Transcript
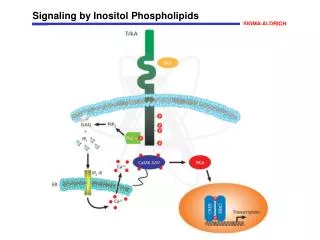
The Biological Basis for the Cardiovascular Consequences of COX-2 InhibitionTilo GrosserInstitute for Translational Medicine and TherapeuticsUniversity of Pennsylvania
Membrane phospholipids a b a b
Differential Inhibition of COX isoforms Grosser et al., JCI, 2006;116(1):4-15
Selectivity for COX-2 is a continuous, rather than a discrete variable COX-1 selectivity COX-2 COX-2 selectivity COX-1 FitzGerald and Patrono NEJM 2002
160 120 80 40 0 A large fraction of human prostacyclin biosynthesis is COX-2 dependent 160 160 120 120 PGI-M1 ± SE (pg/mg Creatinin) 80 80 * † † † † † 40 40 n=7 n=7 n=7 n=12 n=12 n=10 n=50 n=50 n=50 0 0 Placebo Celecoxib 400 mg Ibuprofen 800 mg Placebo Rofecoxib50 mg qd Indomethacin50 mg tid Placebo Rofecoxib25 mg Celecoxib 200 mg McAdam et al. PNAS. 1999;96:272 Catella-Lawson et al.JPET. 1999;289:735. Fries, Grosser, FitzGerald, Gastroenterology 2006; 130:55 1PGI-M = 2,3-dinor-6-keto-PGF1 ; †P<0.01 vs Placebo; *P<0.05 vs Placebo.
3000 3000 2000 2000 1000 1000 0 0 Urinary Thromboxane and Prostacyclin metabolites are increased in acute coronary syndromes 2,3-Dinor-TXB2 2,3-Dinor-6-Keto-PGF1a pg/mg creatinine pg/mg creatinine [pg/ml] [pg/ml] Controls Non-cardiac chestpain Unstable angina Myocardial infarction N = 4 6 16 14 N = 4 6 16 14 Fitzgerald, D.J., NEJM 1986
PGI2 COX-2 COX-1 Thromboxane A2 amplifies platelet activation and recruits additional platelets to the site of clot formation Platelet activation and aggregation TxA2 ? COX-1 Thrombosis
Common carotid artery injury flexible wire wild type knock-out Prostacyclin modulates the bioactivity of Thromboxane 7.5 * 5.0 Urinary 2,3 dinor TxB2 (Fold over basal) 2.5 * 0.0 IP TP IPTP * p<0.05 vs. wild type Cheng et al., Science 296:593, 2002
Mortality * 100 * (12) (10) 80 60 agonist-induced thrombosis (percent mortality) 40 (14) 20 0 TxA2 COX-2Y385F WT COX-2 KO COX-2 disruption and thrombosis Platelet depletion WT 300 COX-2 KO COX-2Y385F * 200 * Platelet counts (x103 / ml) 100 * * 0 ( 12.5 25 Collagen (mg) Cheng Y, et al. J Clin Invest. 2006;116:1391-1399.
P<0.01 P<0.05 vehicle DFU Prostacyclin modulates thrombosis dose dependently 120 100 P<0.01 80 P<0.05 P<0.05 Complete occlusion time (min) 60 40 20 0 vehicle DFU +/+ +/- -/- wildtype IP COX-1 KD Cheng Y, et al. J Clin Invest. 2006;116:1391-1399.
ADP Thrombin TxA2 Thrombosis COX-2 derived prostacyclin acts as a constraint on all thrombotic stimuli
COX-2 inhibition augments thrombosis • COX-2 disruption or inhibition augments the thrombotic response to various stimuli in vivo by depression of prostacyclin biosynthesis. • All coxibs depress prostacyclin biosynthesis = class effect • Suppression of COX-2 dependent prostacyclin does not cause spontaneous thrombosis, but augments the response to thrombogenic stimuli • Hazard from coxibs particularly in those otherwise predisposed to thrombosis ?
Are there differences in hazard between distinct compounds? • Selectivity for COX-2 • COX-2 unrelated effects (“off-target effects”)?
Differential recovery from steady-state inhibition of platelet COX-1 by low-dose Aspirin and Naproxen 100 Aspirin (N = 8) Naproxen (N = 9) 75 50 % Thromboxane inhibition P <.01 P <.01 P =.074 25 0 1 3 12 24 hours after last dose Capone et al., Circulation. 2004; 109(12):1468-71
Opposing roles of COX-2 and COX-1 products in blood pressure regulation and atherogenesis P<0.05 * p<0.05 vs WT; ** p<0.01 vs WT; ## p<0.01 vs WT/Celecoxib 15 P<0.01 150 ** 10 140 * * 130 % lesion area 120 Systolic BP (mmHg) 5 110 ## 100 90 80 0 +/+ TP -/- IP -/- WT WT/Celecoxib COX-2 KO APOE -/- COX-2Y385F COX-1 KD/Celecoxib Kobayashi et al, JCI 114: 784-94, 2004 Cheng et al., J Clin Invest 116; 1391, 2006
Heterogeneity of response to traditional NSAIDs Garcia Rodriguez et al 2005
COX-2 selective NSAIDs vs isoform non-selective NSAIDs • Opposing roles of COX-1 and -2 products in thrombosis, blood pressure regulation and atherogenesis • Non-isoform selective NSAIDs (e.g. naproxen) may afford prolonged platelet inhibition throughout the dosing intervals in some individuals • COX-2 critical in maintaining renal medullary blood flow under conditions of increased vasoconstrictor tone; Hypertension on NSAIDs relates to inhibition of COX-2 • Predisposition to atherosclerosis and hypertension attenuated by coincident inhibition of COX-1 • Differences in the degree of COX-2 selectivity are likely to affect cardiovascular risk
Are there differences in hazard between distinct compounds? • Selectivity for COX-2 • COX-2 unrelated effects (“off-target effects”)?
Celecoxib Rofecoxib Plasma concentration (mM) Plasma concentration (mM) 0.001 0.001 0.01 0.01 0.1 0.1 1 1 10 10 Selection of the drug concentration in hASMC hASMC COX-2 COX-2 COX-1 COX-1 In vivo
High-thruput screen for off-target genomic effects Bas Veh Cel Rof Veh Cel Rof Veh Cel Rof Veh Cel Rof relative expression level high low interleukin 1b -2 hrs 0 hrs 2 hrs 8 hrs 24 hrs All regulated Genes (FDR <0.1) Differentially regulated Genes (FDR <0.1) 3 0 1 3 4
Expression profiles of genes differentially regulated by rofecoxib and celecoxib IL27RA TXNIP TOP3A PTGIS CDK6 LXN PIK3C2B DHRS3 XPO4 GALNT12 KIAA0841 Affymetrix qRT-PCR Affymetrix qRT-PCR
post dose / pre dose ratio high (increase) low (decrease) Metabolomic plasma profiles of celecoxib, rofecoxib are more similar than any drug to placebo compounds known: 92 unknown: 137 median post / pre dose ratio n = 50 healthy subjects Placebo Celecoxib Rofecoxib 200 mg 25 mg Robert Mohney Felice de Jong Metabolon Inc.
Towards an individualization of NSAID therapy Can individuals at risk for CV complications be identified early during treatment?
Interindividual variability in the pharmacological response to COX-2 inhibition Attained COX-2 selectivity 20 10 5 2 Cox-2 selectivity (COX-2 inhibition / COX-1 inhibition) 1 0.5 0.2 Placebo n=50 rofecoxib(25 mg) n=50 celecoxib (200 mg) n=50 Fries, Grosser, FitzGerald, Gastroenterology, 2006 COX-1 activity ex vivo 700 600 500 400 300 Serum TxB2 200 100 hours 0 4 SS 0 SS 4 Single dose steady state COX-2 activity ex vivo 50 40 30 20 Serum PGE2 10 hours 0 4 SS 0 SS 4 Single dose steady state
Genetic contribution to interindividual variability (i) 3000 CYP2C9*3 +/+ 2000 Celecoxib [ng/ml] 1000 0 0 4 8 12 24 36 Time after last dose (hrs) 3000 CYP2C9*3 +/- 2000 Celecoxib [ng/ml] 1000 0 0 4 8 12 24 36 Time after last dose (hrs) Fries, Grosser, FitzGerald, Gastroenterology, 2006
Cardiovascular complications from inhibition of COX-2 relate most plausibly to Inhibition of COX-2 derived prostacyclin formation. Prostacyclin acts as a constraint on all thrombotic stimuli. The cardiovascular hazard pertains to all coxibs and likely to traditional NSAIDs with high COX-2 selectivity. Hazard would be expected to relate to - baseline cardiovascular risk - attained drug selectivity in vivo - dose and duration of exposure - interindividual differences in drug response. High interindividual variability in the pharmacological response to coxibs. Genetic variability in PK and PD contributes to variance.
Garret A. FitzGerald Susanne Fries Yan Cheng Ying Yu Dairong Wang Emanuela Ricciotti