BLINDNESS
BLINDNESS. Presentation by DR.VIOLET (de Sa) PINTO Lecturer, Department of PSM. Objectives:. At the end of the session the student shall have knowledge of :

BLINDNESS
E N D
Presentation Transcript
BLINDNESS Presentation by DR.VIOLET (de Sa) PINTO Lecturer, Department of PSM
Objectives: At the end of the session the student shall have knowledge of : • Blindness :definition, categories of visual impairment, its causes and problem statement • Changing concepts in healthcare with regards to eye care • Prevention of blindness :primary, secondary and tertiary prevention • Vision 2020
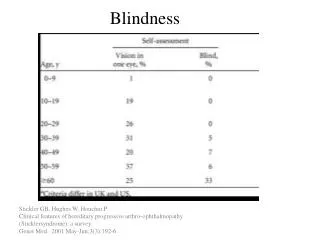
Definition “Visual acuity of less than 3/60 (Snellen) or its equivalent.” Non specialized personnel, in absence of appropriate vision charts “Inability to count fingers in daylight at a distance of 3 meters.”
CATEGORIES OF VISUAL IMPAIRMENTIf it is 6/18 or better = 0 or no visualimpairment
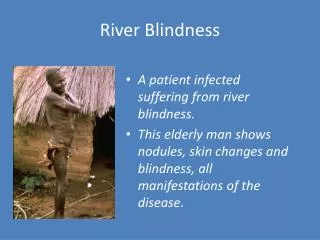
PROBLEM STATEMENT • Estimated 180 million people are visually disabled, nearly 45 million blind, 4 out of 5 living in developing countries. • Major causes…..cataract, glaucoma, trachoma, childhood blindness, onchoceriasis. • 32% are aged 45-59 yrs, large majority 58% are over 60 yrs. • SEAR has 1/3rd of the world’s blind,50% of world’s blind children.
INDIA Causes of blindness • Cataract 62.6% more with advancing age senile cataract- decade earlier • Uncorrected 19.7% Refractive error • Glaucoma 5.8% • Posterior 4.7% segment pathology • Corneal Opacity 0.9% • Others 6.2% Injuries 1.2% cottage industry- carpentry, blacksmitty, stone crushing, chiseling Congenital disorder, uveitis, retina detachment,tumours,diabetes,HT, diseases of nervous system, leprosy.
CHANGING CONCEPTS IN HEALTH CARE Establishment of National Prog. > Need for PHC approach Team Concept Deprofessionalisation VHG, Ophthalmic assistant, MPW, Voluntary agencies Epidemiological Approach Measurement of Incidence, prevalence, risk factors of disease Primary eye care Promotional & protection of eye health On the spot treatment of commonest eye diseases Improve coverage and quality
EPIDEMIOLOGICAL DETERMINANTS AGENT- Trachoma, Vit A def. HOST- Age- About 30% lose eyesight <20 yrs. children and young age group- refractive errors, trachoma, conjunctivitis, Vit A def. Middle age- Cataract, glaucoma& diabetes All ages, 20-40- accidents, injuries Sex- trachoma, conjunctivitis, cataract- More in females, in India
EPIDEMIOLOGICAL DETERMINANTS ENVIRONMENT- • Malnutrition- Vit A def.- even due to measles and diarrhoea PEM related- severe corneal destruction(keratomalacia)6mth- 3yrs.& 4 -6yrs. • Occupation – Cottage industry, workshops, factories, flying objects, gases. Doctors- x rays, u.v. rays, premature cataract • Social class – twice more prevalent in low social classes
PREVENTION OF BLINDNESS The concept of Avoidable blindness (preventable or curable) has gained recognition during the recent years. Initial Assessment Methods of Evaluation Intervention Primary care Secondary care Tertiary care Specific programmes Long term measures Components for action in N.H.P.
1)INITIAL ASSESSMENT • Prevalence surveys – magnitude, distribution, causes • Setting priorities and development of appropriate intervention programmes.
2) METHODS OF INTERVENTION • PRIMARY EYE CARE • Treatment and prevention at grassroot level by locally trained peripheral health worker. (VHG,MPW) (acute conjunctivitis, opthalmia neonatrum, trachoma, superficial foreign body, xeropthalmia) • Provided with essential drugs ; topical tetracycline, Vit A capsules, eye bandages, shields, etc.
Trained to refer difficult cases (eg. Corneal ulcer, penetrating foreign bodies, painful eye conditions & infections which do not respond to treatment) to nearest PHC & district hospital. • Promotion of personal hygiene, sanitation, good diet, safety in general. Currently 1 VHG / 1000 population, 2 MPW / 5000 population.
SECONDARY CARE • Definitive management of common blinding conditions such as cataract, trichiasis, entropion, ocular trauma, glaucoma,etc. • PHC’s and district hospitals where eye departments or eye clinics are established.
Mobile clinics- Disadv- lacks permanence, adv- problem specific best use of local resource, provide inexpensive eye care Eye camp approach- cataract, general eye health, surveys.
TERTIARY CARE • At National /Regional capitals, often associated with Medical colleges & institutes of medicine (National Institute for Blind, Dehradun) • Sophisticated eye care- retinal detachment , corneal Grafting • Eye banks- Maximum states passed Corneal grafting Acts • Education of blind in special schools and utilisation of their services (employment)
SPECIFIC PROGRAMMES • TRACHOMA CONTROL- Endemic trachoma and associated infections, major cause of preventable blindness. • Early diagnosis and treatment • Mass campaigns with topical teracycline • Improvement of SE conditions • TC Programme launched 1963. merged NBCP in 1976. • SCHOOL EYE HEALTH SERVICES- • Screened & treated for refractive errors, squint,ambylopia, trachoma • H.E. – good posture, proper lighting, avoidance of glare, angle between books and eye.
VIT A PROPHYLAXIS 2 lakh IU given 6 monthly 1-6 yrs., surveillance OCCUPATIONAL EYE HEALTH SERVICES Education, protective devices, improve safety of machines, proper illumination, pre placement examination.
3) LONG TERM MEASURES • Improving quality of life, modifying factors responsible for persistence of eye health problems. Poor sanitation , lack of adequate safe water supplies, increase intake of food rich in Vit A, lack of personal hygiene. • Health Education • Create community awareness of the problem • Motivate community to accept total eye health programmes. • To secure community participation. • EVALUATION Evaluation of objectives.
VISION 2020 “A global initiative to eliminate avoidable blindness by WHO on 18th feb.1999.” Objective: Assist member states in developing sustainable systems, which will enable them to eliminate avoidable blindness from major causes.
Plan of Action for country has following features: Target diseases: Cataract, refractive errors, childhood blindness, glaucoma, diabetic retinopathy. H.R.D. as well as infrastructure and technology developmnt. At various levels of health system. Proposed 4 tier system
C.O.E. 20 Training centers Tertiary care including retinal surg.,Corneal transplant. 200 Service Centers 2000 Cataract Surgery Othr common eye surg. Facilities for refraction Referral services Vision Centers 20,000 Refraction and prescription of glasses Primary eye care School eye screening Screening and referral services Prof. leadership, strategy.developmnt, CME,Standards,quality assurance, Research.