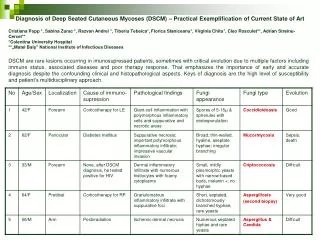
Pediatric Airway Emergencies: Diagnosis and Management of Severe Infections
This comprehensive overview addresses critical pediatric airway emergencies in children aged 2-4 years. Highlighting symptoms such as high fever, rapid onset of distress, stridor, and drooling, the guide emphasizes the importance of early diagnosis and intervention. It covers key conditions like epiglottitis, retropharyngeal abscess, and bacterial tracheitis, discussing common pathogens, recommended antibiotic treatments (e.g., Clindamycin and Ceftriaxone), and potential complications such as respiratory arrest. It underscores the need for skilled ENT consultations and intubation in severe cases.

Pediatric Airway Emergencies: Diagnosis and Management of Severe Infections
E N D
Presentation Transcript
Case 1 • Age 2-4 y/o • High fever, rapid onset • PE: anxious, toxic, muffled voice, drooling, stridor • Posture: tripod, “sniffing position” • Bugs: (Classically H.flu), staph, strep • Abx: Clinda + Ceftriaxone • Dx: Clinically, lat neck thumb sign • Tx: ENT/anesthesia skilled intubation + abx • Comp: Resp arrest (may occur rapidly even if pt seems to be in no distress)
Peritonsillar Abscess • Epiglottitis • Ludwig Angina • Laryngotracheobronchitis • Retropharyngeal Abscess • Bacterial Tracheitis
Case 2 • Age < 3 • Fever, dyspnea, dysphagia, drooling, +/- stridor, resists moving neck (most pain with extension), • may see bulge (50%) on one side of post pharyngeal wall • (median raphe divides space- don’t confuse with peritonsillar abscess) • Dx: Lat neck film: prevertebral space > ½ vertebral body (C1-C3) or > vertebral body C4, • Bugs: GAS, Staph, anaerobes • Tx: Clinda, Surgical drainage, Stat ENT consult • Comp: airway obstruction, track to mediastinum or lateral pharyngeal space (jugular thrombosis), spontaneous drainage with asp pneumonia
Peritonsillar Abscess • Epiglottitis • Ludwig Angina • Laryngotracheobronchitis • Retropharyngeal Abscess • Bacterial Tracheitis
Case 3 • 3mos- 5yrs • URI sx, barking cough, inspiratorystiridor • 75% parainfluenza • Dx: Clinical. May see steeple sign • Tx: supportive, decadron, recemic-epi nebs
Case 4 • Any Age (not common in very young children) • Think about it in older kids and teens • Sore throat, fever, muffled voice, drooling, trismus, ear pain, snoring, swollen tonsil with deviation of uvula • Dx: clinical • Group A strep, s.aureus, anaerobes • Tx: Clinda, consult ENT for possible drainage • Comp: spread to lateral pharyngeal abscess, airway compromise, carotid artery sheath involvement
Peritonsillar Abscess • Epiglottitis • Ludwig Angina • Laryngotracheobronchitis • Retropharyngeal Abscess • Bacterial Tracheitis
Case 5 • Classically age <3, now seen more up to 7y/o • Preceded by viral infxn, usually improves then rapidly becomes toxic appearing (Biphasic) • High fever, purulent cough, +/-stridor and tachypnea, NO drooling, NO neck stiffness, and can lie flat • Staph, resp flora (moraxella, Hflu, anaerobes) • Clinda or VancPLUS Cefriaxone • 50% get intubated • Comp: pneumonia, resp arrest, Toxic shock syn
Ragged tracheal border Pseudomembranes From thick exudates
Peritonsillar Abscess • Epiglottitis • Ludwig Angina • Laryngotracheobronchitis • Retropharyngeal Abscess • Bacterial Tracheitis