Download

1 / 64
660 likes | 894 Views
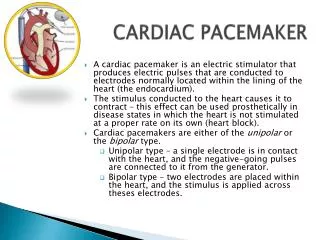
AICD and Pacemaker Update. Kathryn Gray CRNA. Terminology:. Excitability: The ability of a cell to respond to a stimulus by depolarizing and propagating an action potential Depolarization : Occurs when there is a decrease in the polarity across a cell membrane.

E N D
AICD and Pacemaker Update Kathryn Gray CRNA
Terminology: Excitability: The ability of a cell to respond to a stimulus by depolarizing and propagating an action potential Depolarization: Occurs when there is a decrease in the polarity across a cell membrane. Hyperpolarization: Occurs when there is an increase in the polarity across a cell membrane. Conductivity: The ability of a cell to transmit action potentials to adjacent cells. Rhythmicity: The ability of cells to generate automatic action potentials.
Lets get nerdy… This equation is used to define the electrical gradient across a membrane based on ion concentrations This can be applied to cardiac myocytes which helps to explain the ion potentials during AP propagation and RMP.
Paging Dr. Nernst Nernst Equation Em= (-RT/zF) X log [K]i/[K]o Em is the equilibrium potential of the ion based on transmembrane concentrations. R-universal gas constant (8.314472 JXK -1) T- absolute temperature (273.15 degrees kelvin) [K]i- potassium concentration on the inside of the cell [K]o-potassium concentration on the outside of the cell. z- the number of electric charges carried by a single potassium ion F- the Faraday constant (9.6485309 X104 cmol-1)
Lets get really nerdy… The Goldman-Hodgkin-Katz equation accounts for the ionic potentials of multiple ions across a cell membrane. EMF= 61.5 X log([Na]iPNa+[K]iPK+[Cl]oPCl) ([Na]oPNa+[K]oPK+[CliPCl)
The Sinoatrial Node The SA node is made up of specialized cardiac muscle cells which do not have contractile abilities. The SA node is the primary pacemaker in the cardiac conduction system. It’s intrinsic rate is faster than the other latent pacemakers in the heart and thus overrides them. It’s automaticity and intrinsic rate is dependant upon *calcium leak channels in the sarcoplasmic reticulum.
Ectopic Pacemakers This is a portion of the heart with a more rapid rate than the sinus node. Also occurs when transmission from the SA node to A-V node is blocked (A-V block). During sudden onset of A-V block, sinus node impulses do not get through, and next fastest area of discharge becomes pacemaker of heart beat. Delay in pickup of the heart beat is called “Stokes-Adams” syndrome. The new pacemaker is in A-V node or penetrating part of A-V bundle.
AV node The AV node contains highly specialized tissue that slows impulse conduction considerably thereby allowing sufficient time for complete atrial depolarization and contraction prior to ventricular depolarization and contraction.
Purkinje Fibers Located in the inner ventricular walls of the heart, just beneath the endocardium. The Purkinje fibers have the fastest conduction speed of any fibers in the heart.
The ventricles Normal ventricular RMP is -80 to -90mV Action potential is accelerated once threshold is reached by the opening of fast Na channels and slow Ca channels.
Innervation of the heart Releases norepinephrine at sympathetic ending Causes increased sinus node firing rate Increases rate of conduction impulse Increases force of contraction in atria and ventricles Parasympathetic (vagal) nerves, Release acetylcholine at their endings innervate S-A node and A-V junctional fibers Causes hyperpolarization because of increased K+ permeability in response to acetylcholine Muscarinic Acetylcholine Receptors, when stimulated cause decreased heart rate Sympathetic Parasympathetic
Causes of cardiac dysfunction Temperature extremes pH imbalances Hypo or Hypercalcemia Malnutrition, cachexia Hypoxia/Ischemia Hypo or hyperkalemia Autonomic imbalances Hypo or hypercarbia Magnesium deficiency Drug toxicity and adverse drug reactions Stress and catecholamine release CAD HTN Dilated myopathy Morbid obesity Advanced age CHF Chronic lung disease and subsequent corpulmonale Endocrine imbalance Hypertropicmyopathy Sick sinus syndrome Increased ICP Renal disease Physiologic Imbalances Associated Co-motbidities
Types of conduction disruptions • - Atrial Fibrillation • - Atrial Flutter • - 1st degree heart block • - 2nd degree heart block • - 3rd degree heart block • - Ventricular fibrillation • - Ventricular tachycardia • - Re-entry arrhythmias
This is a schematic of how each pacemaker will affect the EKG depending on the intrinsic beat and pacemaker mode
Rate Responsive Pacemakers • Rate-Responsive Direct metabolic sensors: • 1. Mixed Venous O2 saturation • 2. Central venous pH • In-Direct metabolic sensors: • 1. Ventilation rate • 2. Mixed Venous Temperature • Non-Metabolic Physiological sensors • 1. QT interval • 2. Ventricular Depolarization Gradient • 3. Stroke Volume • 4. Mean Arterial Blood Pressure • Direct Activity sensors • 1. Motion detection
Anesthesia and in situ pacemakers Electromagnetic interference is always a problem when taking a person into the OR for a surgical procedure. Increase in Pacemaker threshold with some drugs in the OR setting. Physiologic alterations can change pacemaker function.
Questions you need to ask before going into the OR What is the device? What brand and model? Does your hospital have a programmer for this make and model? What is the magnet mode? Why does the patient have a pacemaker? What rhythm does the patient have when the pacemaker is shut off? When was the last time it was interrogated? How long has it been since the battery has been changed?
IT DEPENDS!! • What do you do when your patient has an existing pacemaker or AICD?
Anesthesia for patients with AICD’s Questions to ask the patient: Why do they have an AICD? How long have they had it? Who is the manufacturer? When was the last time it was interrogated? When was the last time they received an AICD shock? How often do they get shocked?
Electrocautery Bipolar vsUnipolar Why do we need a grounding pad? Why are we afraid of bovie with pacemakers and AICD’s?
Electromagnetic interference in the O.R. Electrocautery MRI ESWL Defibrillation Motor evoked potentials Nerve stimulators
Oversensing • Cause • Insulation breach • Bipolar impedance