Download
1 / 41
450 likes | 744 Views
Dynamic simulation of mitral valve using the Immersed boundary method. Dr. Xiao Yu Luo Department of Mathematics University of Glasgow Glasgow, G12 8QW UK. Acknowledgement. Dr. Paul Watton, Mr. Min Yin Dept. of Mathematics, University of Glasgow. Professor Wheatley, Dr. G. Bernacca

E N D
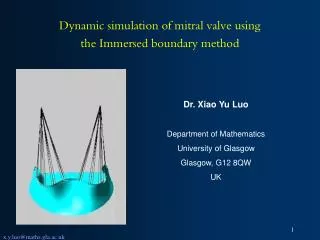
Dynamic simulation of mitral valve using the Immersed boundary method Dr. Xiao Yu Luo Department of Mathematics University of Glasgow Glasgow, G12 8QW UK
Acknowledgement Dr. Paul Watton, Mr. Min Yin Dept. of Mathematics, University of Glasgow. Professor Wheatley, Dr. G. Bernacca Dept of Cardiac Surgery, University of Glasgow, Glasgow, UK Professor Xiaodong Wang Department of Mathematical Sciences, New Jersey Institute of Technology.
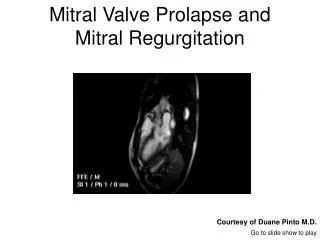
Anatomy of a mitral valve (MV) • MV: two leaflets, anterior leaflet (larger), and posterior leaflet (smaller). • Chordae run from valve leaflets to papillary muscles at the base of ventricle.
(Mitral valve) MV: top view The chordae reinforce the leaflet structure and prevent prolapse of the leaflets. They also assist in maintaining the geometry and functionality of the ventricle.
MV diseases • Typical diseases of MV: Mitral stenosis & mitral regurgitation. • MV needs to be repaired or replaced when damaged. • Two types of valve replacements: mechanical and bioprosthetic valves.
Mechanical mitral valves Generation 1: (A) Starr-Edwards ball-and-cage. 2: (B) Medtronic-Hall tilting-disk, (C) Omnicarbon tilting-disk. 3: (D) St. Jude Medical bifleaflet, (E) Carbomedics bileaflet. (F) ATS bileaflet. (G) ON-X bileaflet. All require life long anticoagulant therapy, even the best designs have risks of hemorrhage related to anticoagulant therapy and thromboembolism
Bioprosthetic mitral valves. Generation 1: (A) Hancock II porcine heterograft, 2: (B) Carpentier-Edwards standard porcine heterograft, (C) Mosaic porcine heterograft. 3: (D) Carpentier-Edwards pericardial bovine heterograft. 20% failing with 10 years. Rate of deterioation accelerates for young patients.
Current designs offer no ideal substitutes Use of aortic valve design, and put in reversed configuration: Potential of changing the vortex structure in the flow inside the ventricle. Have no chordae attached: Potential of changing the ventricle wall mechanics, and causes prolapse. Clinical observation: The durability of porcine valves is less with mitral bioprostheses than with aortic bioprostheses.
A New Bioprosthetic Mitral Valve A new bioprosthesis (polyurethane) design developed by Dept. of Cardiac Surgery, University of Glasgow • Benefits: • durable • no need for anticoagulation therapy, • biostable (tested on sheep) • based on real MV geometry, similar mechanical property, • with chordae for the first time. D.J. Wheatley (2002), Mitral valve prosthesis Pat. no. WO03037227.
Evaluating the new MV design using simulations • A key question is what happens when inserted in the ventricle? • We test this design dynamically using the Immersed boundary (IB) method.
X(r,t) s s r: fibre point coordinates, T: tension x: fluid coordinates, Immersed Boundary (IB) Method Fluid: t Solid: Interactions: where solid behaves like fibres immersed in the fluid. It imposes force f on the fluid, and is moved by the fluid.
N4 N3 N2 N1 Generating Fibres The valve is represented by 4 node quadrilateral elements made of 2 fibres, each with three nodes. Fibre 2 Each fibre is modelled as a Hookean spring: Fibre 1 where s =fibre stiffness, E=Young’s modulus, A=cross-sectional area, l= fibre resting length, l=fibre stretch, T=tension.
The tethering fibres where, u(r,t) is the velocity of the fibres. Note if two nodal points on two different fibres have identical spatial positions at t=0, then this will be true for all successive times. Tethering fibres with a great stiffness, make use of this fact to enforce boundary conditions.
Smooth approximation of Delta function h: grid size Fluid: on a fixed Eulerian grid, Solid: network of fibres on a Lagrangian mesh.
Solving Fluid equations with FFT • The matrix equation of the discretized Navier-Stokes equations are Kun+1=F(un) where unis the solution vector at the nth time step. • This is linear in un+1, thus can be solved using the Fast Fourier Transform method (recall that the Eulerian grid is uniform). • In other words, we now need to have periodic boundary conditions.
2) Distribute Fibre Force to Fluid Grid Points 1) Compute fibre force density, F 4) Evolve fibres at the new local fluid velocity 3) Solve Navier-Stokes Equations (FFT) ALGORITHM
SOLIDWORKS (Valve Design) The IB valve modelling GAMBIT (Mesh Software) FIBRE GENERATOR IB CODE MATLAB (Graphics) a b c Export: mesh files for (a) leaflets; (b) chordae; (c) fixed boundaries.
CAP CAP Chordae attached to the leaflets 14 chordae total • Anterior only (b) with posterior • CAP=Chordae Attachment Points
The IB Model • Cylindrical Tube: Length 16cm Diameter 5.6cm. • Experimentally determined periodic velocity profile prescribed. • Viscosity: 0.01g/m.s Density: 1g/cm3 • Submerged within a fluid mesh: size 64x64x64
Validations – Static Aortic Valve E=15MPa, h = 0.125mm Polyurethane material • Valve housed in experimental rig and subject to an incremental steady pressure. • Displacement of centre of 3 leaflets measured and compared with IB results. • Good quantitative comparison for deformation obtained.
Validations -Static Mitral Valve ANSYS IB P=120mmHg. Leaflets: E=4.29MPa, H = 1.32mm, Chordae: E=47MPa, A = 0.4mm2. Colormaps of surface displacements (mm) • Model based on Kunzelman’s model of native mitral valve. • Deformation and peak stress predicted by IB and ANSYS in agreement.
IB versus ANSYS • IB is much better with thin structures. Ansys has “locking” phenomenon, hence a thicker shell has to be used (increasing thickness by 3-4 times, while reducing Young’s modulus by the same scale). • IB is fast • IB is designed for dynamic modelling. Ansys is not. • Current IB has no bending. • Current IB is not so good with contact problems.
Validations: Dynamic MV with fixed CAP Flow Rate (ml/s) Time (s) Experimentally determined flow profile prescribed. Polyurethane leaflets: E = 5MPa, h = 0.125mm Chordae: E = 30MPa, Area = 0.4mm2 NOTE: Chordae are in leaflet surface in computational model but not visually represented. • Computation model of valve behaves too flexibly. • Unrealistic crimping of leaflets occurs. • IB unable to model bending effects.
Exp. mmHg IB mmHg Validations: Pressure Gradient, fixed CAP Pressure Gradients Given Flow Profiles mmHg Predicted pressure gradients consistent with experimental ones. However, note a higher (and delayed) peak pressure in IB.
Physiological Chordae Attachemnt Points (CAP) motions • Analyse Human MRI data with CMRTOOLS - software package for analysing Cardiovascular Magnetic Resonance (CMR) images (Imperial College www.cmrtools.com) • Determine dynamic geometry of ventricle and papillary muscle axes. • Intersection of data enables papillary muscle regions of ventricle to be identified
Track Mitral Annulus DIASTOLE SYSTOLE • Software package Slice-o-Matic used to analyse MRI data. • Tracks motion of Mitral Annulus through 2 planes (32 Time Slices of Data) • Note relative displacement of mitral annulus plane to apex of ventricle is obtained.
Determining Motion of Mitral Apparatus • CMRTOOLS - Determine geometry of ventricle and papillary positions. • Slice-O-Matic - Track 4 points on mitral annulus. • Fortran code - Convert CMRTOOLS data to Matlab surface data. • Matlab scripts - 1) Transform Slice-O-Matic and CMRTOOLS data to common coordinate system. • 2) Tag papillary attachment regions on ventricle. • 3) Determine relative motion of mitral apparatus.
Relative Motion of CAP to Annulus Relative motion to a fixed annulus CAP=Chordae Attachemnt Point, which will be the attachment point to the ventricle during surgery. The relative motion of CAP to mitral annulus is determined. Only perpendicular direction is considered. The averaged distance-time curve from the 4 points are used for the two CAP positions.
Physiological Boundary Conditions Experimental Flow Rate Flow prescribed at the tube entrance and exit. Pressure gradient (calculated). Relative CAP motion is prescribed perpendicular to the mitral annulus plane. ml/s Valve opens Pressure Gradient mmHg Onset of systole mm Physiological CAP motion Time (s)
Pressure Gradients Opening pressure gradient reduces with CAP motion.
Leaflet stretches with CAP motion Anterior: circumferential Anterior: longitudinal Posterior: circumferential Posterior : longitudinal ANTERIOR: small difference, POSTERIOR: stretches increase.
Chordae Stretches No ANTERIOR CHORDAE Stretch POSTERIOR CHORDAE Stretch • Anterior leaflet can accommodate the CAP motion without its chordae becoming taut • CAP motion results in high stretches of the posterior chordae (lower right). • NOTE: Stretches <1, denote chordae relaxed.
Up to 20% strain increase due to papillary motion • Anterior leaflet can accommodate CAP motion. • Posterior leaflet subject to significantly higher stretches detrimental effect on the long-term durability of the valve.
Ongoing work To add ventricle model to model detailed flow and vortex.
Ongoing work Improvements for IB code: • Developing a better solid model with bending stiffness. • Use adaptive mesh to get rid of sticking effects when opening. • Better boundary conditions.
Summary • Dynamic analysis for a mitral valve with chordae attachment points (CAP) moving with ventricle is carried out with a IB code. Results show that: • CAP motion assists the opening of the valve (lower opening pressure gradients). • Current design: posterior is over-stretched. • Recommendation for design improvements: • Modify geometry to allow a greater movement of the posterior leaflet. • Modify stiffness of posterior chordae: low modulus external chordae that can accommodate high stretches, and high modulus internal leaflet chordae, which resist deformation • Design a stiffer posterior leaflet which does not require chordae.
Locking in FEM Where thickness parameter is the unknown solution, is the scaled bending energy, is the scale membrane energy, is the scaled external virtual work. If r=3, bending-dominated r =1, membrane-dominated ill-posed membrane problem
Fibre Representation of Prosthetic Mitral Valve Fibres generated automatically from an FEM mesh. Stiffness dependent on valve material and element sizes.
Smooth approximation of Delta function h: grid size
Leaflet stretches with CAP motion Anterior: circumferential Anterior: longitudinal Posterior: circumferential Posterior : longitudinal ANTERIOR: small difference, POSTERIOR: stretches increase.