Download
1 / 59
610 likes | 881 Views
Türk Toraks Derneği 11. Annual Congress FEMTOS Session 23 - 27 April 2008 Maritim Pine Beach Resort - Antalya. Sleep Center Organisiation and Managment. Doç. Dr. Sadık Ardıç SB Dışkapı Eğitim ve Araştırma Hastanesi Göğüs Hastalıkları ve TBC Kliniği

E N D
Türk Toraks Derneği 11.AnnualCongress FEMTOS Session 23 - 27 April 2008 MaritimPineBeachResort - Antalya Sleep Center Organisiation and Managment Doç. Dr. Sadık Ardıç SB Dışkapı Eğitim ve Araştırma Hastanesi Göğüs Hastalıkları ve TBC Kliniği Uyku Hastalıkları Tanı ve Tedavi Merkezi
Dr. Karacan’ın örgütlenmesi doğru, benim ki doğru değil. Sleep Disorders Centers,Baylor College of Medicine, 10.9.1992
SleepCenterOrganisiationandManagment • SleepDisordersCenter(SDC) • Inthesecenters, All of SleepDisordersarebeendiagnosedandtreated. • SDC is managedbyMedicalSleepSpecialistswhichhavestudiedsleepmedicine
Sleep Center Organisiation and Managment • SleepDisordersCenter is described as a unitwhich is an individualand a separatelocation.. • Personnelswhichwork in SDC,respecttheethics of sleepdisorders.
Sleep Center Organisiation and Managment • Medical Director(MD) • Medical Director has been a Medical Doctor. • Medical Sleep Specialists: • The certificate intends to show that the named person is able to carry out the diagnosis and differential diagnosis of sleep-related diseases, as listed in ICSD-2 (2), and their management.
Sleep Center Organisiation and Managment OtherPersonnels • SleepTechnician (ST) • ST is abletocarryouttheorganization, logistics, preparation, recording, observation, analysis & evaluationanddocumentation of polysomnography(PSG) andotherinvestigationscarriedout in the SMC. • ST is responsibleforthecorrectinstructionandcare of thepatients
Sleep Center Organisiation and Managment OtherPersonnels • SleepTechnician (ST) • ST is abletoscorethepolysomnographicrecordbymanually • STmustreceive a trainingduring a full time equivalentperiod of thedescribedtime in an accreditedSleepDisorderCenter
Sleep Center Organisiation and Managment Rooms; • Rooms;minimum bedroom surface of 10-12 m2 is recommended. • SDC has two bedrooms at least.
Sleep Center Organisiation and Managment • The following criteria must be met for the approval of a polysomnographic bed: • Only those beds that are located in single bedrooms and , • in which the polysomnograph allows recording of all relevant biosignals will be approved as polysomnographic beds.
Sleep Center Organisiation and Managment • The bedrooms must be equipped to allow Professional diagnosis and therapy in the field of sleep medicine to be carried out and to enable both nocturnal examinations and assessment of daytime sleepiness
Sleep Center Organisiation and Managment • The rooms must be sound and light attenuated and equipped with temperature and ventilation controls. • To enable daytime assessments, such as the multiple sleep latency test (MSLT), the rooms must be adequately darkened.
Sleep Center Organisiation and Managment • Adequate sanitary facilities must be available near the bedrooms. • Each bedroom should be equipped with a suitable video monitoring system. • A two-way communication system must be installed which allows the patient and night duty technician to communicate with each other, and to enable biosignal calibration. • Disabled people should be examined in these rooms
Sleep Center Organisiation and Managment • Control Room • It is been at the same floor which the bed rooms are. • Its location must be The central of Sleep Lab, • Its distance to each room must be equal
Sleep Center Organisiation and Managment • Control Room • A two-way communication system must be installed which allows the patient and night duty technician to communicate with each other, and to enable biosignal calibration.
Sleep Center Organisiation and Managment • Control Room • A separate room, which is also sufficiently large and • Which ensures undisturbed working conditions, must be available for the monitoring equipment and the technical/nursing staff.
Sleep Center Organisiation and Managment LaboratoryGuideManuel(LGM) • Theremust be a LGM which has to be describedall of procedureandapplication in SDC. • Thisbookdescribesall of thedaillyprocedure in SDC. • Thisbook is a referencebookforsleeptechnician(ST) whoapplyforeverythingandproblems in SDC.
Sleep Center Organisiation and Managment • LaboratoryGuideManuel(LGM) • It has toshowall of thedetails of testswhich PSG,CPAP titration, MSLT,Epilepticfollowup • It has toshowallprocedureswhenthepatient is accepted SDC. • SDC mustfollowthenationalsleepsocietyguidemanuel.
Baylor Collage of Medicine,Sleep Disorders Center Houstun-Texas, USA- 1992
Uyku Laboratuvarı Standartları Equipment: Each Room has to be connected PSG which has sixteen channels (6 EEG, EOG, 3 EMG) PSG has AC channels and DC channels. At the same time DC channels are able to record.
Sleep Center Organisiation and Managment Equipment: • PSG has Respiratory channels,oxymeter, ECG,leg EMG,body position sensor, microphone • Polisomnographic records(all nights)has to be evaluated 30 or 60 second epochs.
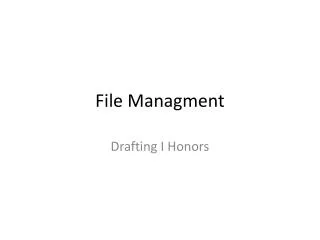
C4A1 O2A1 C3A2 O1A2 ROG LOG CHIN-EMG EKG RLEG LLEG
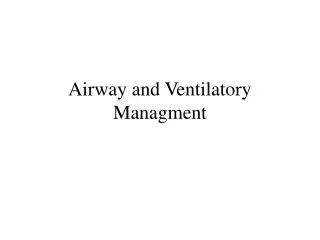
EEG: Zemin; nispeten düşük voltaj, karışık frekans, Uyku iğciği 12-14 cps (>0.5 sn) K Kompleks EOG: Arasıra SEM, EMG: Tonik aktivite düşük düzeyde
EEG: Nispeten düşük voltaj, karışık frekans, Teta aktivitesi, yavaş Alfa, testere dişli dalga EOG: Fazik REM, EMG: Tonik supresyon, fazik dönemler
Sleep Center Organisiation and Managment • Minimum montage for standard sleep medicine polysomnography • 6 EEG (e.g. F4-M1,C4-M1,O2-M1 or F3-M2, C3-M2, O2-M2) • 2 EOG • 3 mentalis/submentalis EMG • SaO2 • Snoring signal • Body position sensor • Nasal pressure/flow signal (thermistors are no longer acceptable as a single recording method in adults) • Validated method of respiratory effort • 2 EMG, tibialis anterior • ECG, one channel • Video monitoring with possibility of recording
POLİSOMNOGRAPHY • EEG, EOG, EMG • (Submental) • Oro-NasalAirflow • RespiratoryEffort • Channels • Oxymeter • ECG • EMG (Tibial) • Body Position Sensor • Microphone
Sleep Center Organisiation and Managment Recording in SMC, • In SMC, the ongoing recording should be monitored by trained technical or nursing staff who MD is responsible from . • SDC has to have atleast two Sleep Technicians who has their knowledge of and experience in sleep medicine. Each ST is responsible from two patient.
Sleep Center Organisiation and Managment Recording in SMC, • Polysomnography (PSG) technologists for nocturnal and diurnal recordings are required to ensure the proper, artefactfree functioning of the recording devices, to detect problems and resolve them. • This makes their presence during the entire recording process an absolute necessity. • Between Night and Daytime technicians’s working schedule will be planned consistenly
Sleep Center Organisiation and Managment • Diagnostic tests • Additional diagnostic tests that are routinely performed at the SMC should be listed here, e.g. • Physical examination • Clinical investigations (e.g. laboratory analyses, radiology, pulmonary function tests, etc.) • MSLT, • MWT • Sleep diary
Sleep Center Organisiation and Managment • Diagnostic tests • Sleep questionnaires [e.g. Pittsburg Sleep Quality Index(PSQI), Epworth Sleepiness Scale (ESS), Stanford Sleepiness Scale (SSS), etc.] • Psychological and personality questionnaires (e.g. MMPI, etc.) • Neuropsychological examinations (vigilance, psychometric and cognitive tests) • Other.
Sleep Center Organisiation and ManagmentIn polisomnography which parameters are been recorded? Sleep Parametres • EEG • EOG • EMG • EKG
EEG -Recommended • F4-M1 • C4-M1 • O2-M1 F3, C3, O1 and M2 derivations are placed backupelectrods If there is necessary to use backup channels for PSG record. • F3-M2 • C3-M2 • O2-M2
EOG; Recommended LOC E1-M2 (E1;Left outer cantus lower 1 cm) E2-M2 (E1;Right outer cantus above1 cm) ROC
Sleep Stages • W: ‘’Wakefullness’’ • N1: ‘’NREM 1’’ • N2: ‘’NREM 2’’ • N3: ‘’NREM 3’’ (NREM3 and 4 combined) • R : ‘’REM’’ • 30 sn epoch • If there is multiple sleep stage in an epoch,that the longer stage is scored .
Sleep Center Organisiation and ManagmentIn polisomnography which parameters are been recorded? • Respiratory parameters • Oro-nasal airflow • Respiratory Effort(Thoracic and Abdominal effort) • Oxygen Saturation • Snoring and respiratory sounds • CO2 measurement • Intra thoracic effort