Download
1 / 36
360 likes | 371 Views
Behavioral and Biological Risk Factors of Non Communicable Diseases. Prof. Dr. M. S. A. Mansur Ahmed Professor Dept. of Public Health DIU. Global scenario of NCD. Of 56 million global deaths in 2012, 38 million, or 68%, were due to noncommunicable diseases.

E N D
Behavioral and Biological Risk Factors of Non Communicable Diseases Prof. Dr. M. S. A. Mansur Ahmed Professor Dept. of Public Health DIU
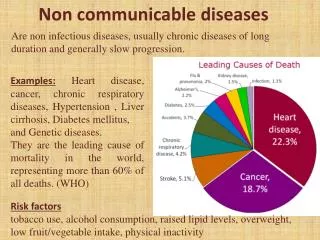
Global scenario of NCD • Of 56 million global deaths in 2012, 38 million, or 68%, were due to noncommunicable diseases. • The four main NCDs are cardiovascular diseases, cancers, diabetes and chronic lung diseases. • The burden of these diseases is rising disproportionately among lower income countries and populations. • In 2012, nearly three quarters of noncommunicable disease deaths -- 28 million -- occurred in low- and middle-income countries with about 48% of deaths occurring before the age of 70 in these countries.
Leading causes of NCD deaths in 2012 • The cardiovascular diseases (17.5 million deaths, or 46% of all NCD deaths), • cancers (8.2 million, or 22% of all NCD deaths), and • respiratory diseases, including asthma and chronic obstructive pulmonary disease (4.0 million). • Diabetes caused another 1.5 million deaths.
Contd. • The importance of addressing noncommunicable diseases at the global level has also become a major element of the ongoing discussion concerning the post-2015 development goals, which is being steered by the United Nations. • Noncommunicablediseases were omitted from the Millennium Development Goals in 2000, • A consensus is emerging among the various United Nations agencies and other international organizations that • A life-course perspective must be adopted, with an emphasis on noncommunicable diseases as part of the health goal to be included in the set of post-2015 Sustainable Development Goals.
Bangladesh scenario • NCDs have already appeared as a major public health problems. • Major NCDs (DM,CVDs,Cancer,COPD &Accidents)were among the top twenty causes of deaths in 2000(BBS 2000).
NCD risk factor survey 2010 • NCD may account for 61% of the total disease burden. • Among adults(15+years) 97% had at least one risk factor half of whom had 2 risk factors. • 40 million (app.25%) people are tobacco users • 17 million (nearly 20%) are not doing adequate physical activities. • 18% adults with Hypertension • 4% documented Diabetes.
Table 1: Findings of Bangladesh NCD risk factor Survey 2010 at a glance. Prevalence (%) with selected risk factors among the adult population aged ≥25 years
Behavioral and Biological Risk Factors of Non Communicable Diseases • Behavioural risk factors, including tobacco use, physical inactivity, and unhealthy diet, are responsible for about 80% of coronary heart disease and cerebrovascular disease.
Biological risk factors Biological risk factors comprise • raised blood pressure, • raised blood glucose, • raised total serum cholesterol, • Dyslipidemia • overweight and obesity, • fat intake and • salt intake.
Current status and trends in risk factors • Common, preventable risk factors underlie most NCDs. These risk factors are a leading cause of the death and disability burden in nearly all countries, regardless of economic development. • The leading risk factor globally for mortality is: • raised blood pressure (responsible for 13% of deaths globally), • followed by tobacco use (9%), • raised blood glucose (6%), • physical inactivity (6%), • overweight and obesity (5%).
Current status and trends in risk factors contd. • The prevalence of these risk factors varied between country income groups, with the pattern of variation differing between risk factors and with gender. High-, middle- and low-income countries had differing risk profiles. • Several risk factors have the highest prevalence in high-income countries. These include: • physical inactivity among women, • total fat consumption, • raised total cholesterol. • Some risk factors have become more common in middle-income countries. These include: • tobacco use among men, • overweight and obesity.
Parameters for estimation of behavioural and metabolic risk factors current daily tobacco smoking: the percentage of the population aged 15 or older who smoke tobacco on a daily basis. physical inactivity: the percentage of the population aged 15 or older engaging in less than 30 minutes of moderate activity per week or less than 20 minutes of vigorous activity three times per week, or the equivalent. raised blood pressure: the percentage of the population aged 25 or older having systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥90 mmHg or on medication to lower blood pressure.
contd. raised blood glucose: the percentage of the population aged 25 or older having a fasting plasma glucose value ≥ 7.0 mmol/L (126 mg/dl) or on medication for hyperglycemia. overweight: the percentage of the population aged 20 or older having a body mass index (BMI) ≥ 25 kg/m2. obesity: the percentage of the population aged 20 or older having a body mass index (BMI) ≥30 kg/m2. raised cholesterol: the percentage of the population aged 25 or older having a total cholesterol value ≥ 5.0 mmol/L (190 mg/dl).
BANGLADESH MEDICAL RESEARCH COUNCIL • Project Title: Prevalence of NCD Related Risk Factors Among Population Aged 35-60 in Dhaka City. • Principal Investigator(s): Prof. Dr. M. S. A. Mansur Ahmed, Head, Dept. of Community Medicine, Bangladesh Institute of Health Sciences, Dhaka. • Co-investigator(s): • Dr. Md. Shahjahan, Assistant professor, Dept of Epidemiology and • Biostatistics, BIHS, Dhaka. • 2. Mr. Moniruzzaman ,Senior Research Fellow, Dept. of Community Medicine, • BIHS, Dhaka. • Place of the study/ Institution(s): Bangladesh Institute of Health Sciences • Date of Commencement: January, 2011 • Date of Completion: June, 2011
Table 1. Distribution of respondents according to their socio-demographic characteristics (n=400).
Smoking habit • About 25 percent of the respondents were currently exposed to smoking during time of conducting the survey. • The mean number of stick per day was 10 with SD ±6 (Table 2).
Table 2. Distribution of respondents according their smoking habits (n= 400).
Figure 1. Distribution of the respondents according to the habit of smokeless tobacco consumption (Betel nut, Zarda and Gool)
Table 3. Distribution of respondents according to the habit of alcohol consumption (n=400).
Table 4. Distribution of respondents according to the status of doing physical exercise (n=400).
Figure 2: Distribution of the respondents according to BMI categories (n=400)
Table 5: Number of servings of fruits taken by the respondents per day
Table 6: Number of servings of vegetables taken by the respondents per day
Conclusion • Majority of the study population are in economically productive age group. • Mean Duration of smoking was found to be17.58± 9.0 yrs and the mean number of stick perday was 10 with SD ±6 compared to higher rates in some industrialized and developed countries • About one third of the respondents reported doing any form of physical exercise. Among them, 22% maintained recommended physical exercise (minimum 30 min of physical exercise for at 5 days a week). • The recommended fruits intake of at least 5 servings per day by respondents was very low (0.2%).and the recommended vegetable intake of at least 5 servings per day by respondents was very low (1.2%). • Building awareness for behavioral and lifestyle related risk factors should be an agenda for advocacy of the policy planners. • Further studies needed.
CARDIOVASCULAR RISK ASSESSMENT AMONG URBAN POPULATION AGED 40-70 YEARS USING WHO/ISH RISK PREDICTION CHART • SPONSOR: MINISTRY OF SCIENCES AND TECHNOLOGY,GOV’T OF BANGLADESH • Principal investigator: Prof. Dr. M. S. A. Mansur Ahmed, Dept. of Community Medicine,BIHS • Co-investigators • Dr .Shahanaz Choudhury, Asstt.professor, Community Medicine,BIHS • M.Moniruzzaman,Sr. Lecturer, Community Medicine, BIHS • NAME AND ADDRESS OF THE CONTRACTING INSTITUTE: • Bangladesh Institute of Health Sciences (BIHS) • Duration of the Project: 1 year • Date of Commencement: July 2012 • Date of Completion: June, 2013
Table 2:Distribution of respondents according to History of Behavioral Risk Factors (n=150) *1 servings= 80 gm
Table 4:Distribution of respondents according to Physical Measurement (n=150) *BMI – Asian cut off has been used
CONCLUSION • About 19% of the study population are at moderate to high risk of developing CVD event in next 10 years. • The proportion of CVD risk calculated by the chart may be higher if we include other known risk factors (over wt/obesity, physical inactivity, inadequate fruits and vegetable intake, use of extra table salt etc).
TITLE: CARDIOVASCULAR RISK ASSESSMENT AMONG URBAN AND RURAL POPULATION AGED 40-70 YEARS USING WHO/ISH RISK PREDICTION CHART Principal investigator: Prof. Dr. M. S. A. Mansur Ahmed, Dept of Community Medicine,BUHS Co-investigator: 1, Dr. Shahanaz Choudhury,Asst Prof., Dept of Community Medicine,BUHS. 2. M.Moniruzzaman,Sr.Lecturer, Dept.of Community Medicine,BUHS Sponsor: Ministry of Science and Technology, Gov’t of Bangladesh NAME AND ADDRESS OF THE CONTRACTING INSTITUTE: Bangladesh University of Health Sciences (BUHS), 125/1 Darus Salam, Mirpur 1, Dhaka 1216. Duration of the Project: One year Date of Commencement: July 2013 Date of Completion: June, 2014
Table 2:Distribution of respondents according to History of Behavioral Risk Factors (N=508)
Table 4:Distribution of respondents according to Physical, Biological and biochemical Measurement (N=508) *BMI – Asian cut off has been used, **BMI-Body Mass Index
CONCLUSION • Overall 17.5% of the study populations are at moderate to high risk of developing CVD event in next 10 years. • The proportion of high risk was more in rural (11.7%) area than in urban (8.7%) area where as the proportion of moderate risk was more in urban (10%) area than in rural (4.7%) area. • However, the proportion of moderate to high risk was almost similar in urban (18.7%) and rural (16.4%) area.
References • April 2011 the World Health Organization (WHO) report. • Bulletin of the World Health Organization 2013;91:650-660. doi: http://dx.doi.org/10.2471/BLT.13.117549 • Ahmed, MSA M,Shahjahan M, MoniruzzamanM,Prevalence of NCD Risk Factors. BMRC project report,2011. • Ahmed,MSA M, Choudhury S,Moniruzzaman M.Cardiovascular Risk Assessment Among Urban Population Aged 40-70 Years Using WHO/ISH Risk Prediction Chart. Ministry of Science & Technology,Gov’t of Bangladesh, Project report 2013 • Ahmed,MSA M, Choudhury S,Moniruzzaman M.Cardiovascular Risk Assessment Among Urban And Rural Population Aged 40-70 Years Using WHO/ISH Risk Prediction Chart.Ministry of Science & Technology,Gov’t of Bangladesh, Project report 2014 • http://www.who.int/gho/ncd/mortality_morbidity/en/, WHO Global health data, morbidity and mortality 7. Hunter DJ, Reddy KS, Noncommunicable Diseases, N Engl J Med 2013; 369:1336- 1343October 3, 2013DOI: 10.1056/NEJMra1109345