Download
1 / 31
410 likes | 1.11k Views
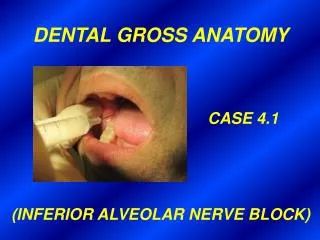
DENTAL GROSS ANATOMY CASE 1 CAVERNOUS SINUS THROMBOSIS. HISTORY Patient develops a boil on his upper lip after cutting himself shaving on a hunting trip He presents to his physician with a high fever and severe headaches

E N D
DENTAL GROSS ANATOMY CASE 1 CAVERNOUS SINUS THROMBOSIS
HISTORY • Patient develops a boil on his upper lip after cutting • himself shaving on a hunting trip • He presents to his physician with a high fever and • severe headaches • Patient does not improve with penicillin injections and • is admitted to a hospital • EXAMINATION • Rigidity of neck muscles • Upper lip swollen and oozing pus • Cheek, side of nose and eyelids swollen • Exophthalmos • Edema of optic nerve at papilla • Inability to move eye • Paresthesia of forehead, side of nose and upper cheek • Blood culture positive for Staphylococcus aureus
DIAGNOSIS • Staphylococcic infection of upper lip and infectious • cavernous sinus thrombosis • THERAPY AND FURTHER COURSE • Patient is put on intravenous antibiotics • Warm, moist dressings applied to face • Narcotics given for pain • Patient responds slowly to antibiotics and ocular • functions improve only gradually • After three weeks patient has made a complete recovery • and is discharged
Where is the cavernous sinus • located?
What anatomical features • does the cavernous sinus • share with other venous • sinuses and in what respects • does it differ?
Cavernous sinus Optic chiasm Hypophysis Differences from other sinuses • Similarities with • other sinuses • Within dura III IV Int. carotid a. (w/sympathetic plexus) Lined by endothelium Lacks muscular coat VI Lacks valves V1 V2 Contains trabeculae Sphenoid sinuses within body of sphenoid bone
3a. What are the tributaries to the cavernous sinus? b. What veins directly drain the cavernous sinus?
Tributaries Cavernous sinus Sup. ophthalmic v. Inf. ophthalmic v. (not shown) Intercavernous sinus Central v. of retina (inside optic n.) Sphenoparietal sinus Superficial middle cerebral v. Drainage Sup. petrosal sinus Inf. petrosal sinus
3c. Into what vein does the blood in the cavernous sinus ultimately drain?
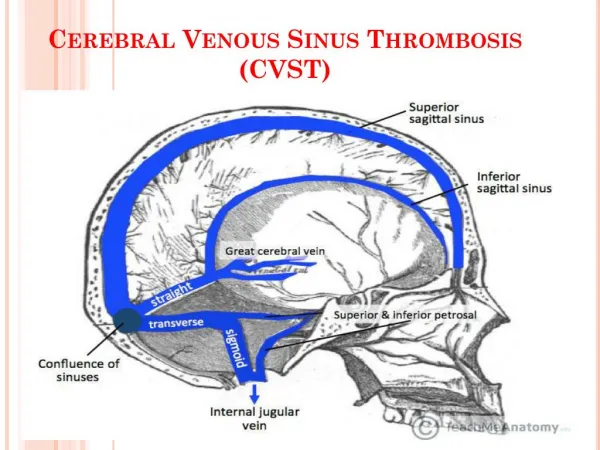
Sup. petrosal sinus Inf. petrosal sinus Sigmoid sinus To int. jugular v.
4a. What is the definition of an emissary vein? Can the ophthalmic veins be regarded as emissary veins? b. What is the direction of blood flow in emissary veins? c. In view of your answer (to b) above, what is the clinical significance of emissary veins?
Angular v. Sup. ophthalmic v. Cavernous sinus Facial v. Inf. ophthalmic v.
Describe the venous pathway • by which infectious material • reached the cavernous sinus • in this patient.
Sup. ophthalmic v. Angular v. Facial v. Sup. labial v.
6. How do you explain the swelling of the eyelids and conjunctivae, the exophthalmos, the dilation of the retinal veins and the edema of the optic nerve in this patient?
Retinal v. Optic n. Central v. of retina
Optic disc (papilla)
What cranial nerves have been • affected by this infectious • thrombosis? (Give reasons for • your answers). Through what • openings do these nerves leave • the cranial cavity?
SO4, LR6, R3 Levator palpebrae superioris m. Sup. oblique m. Sup. rectus m. III IV VI Inf. rectus m. Inf. oblique m. Med. rectus m. Lat. rectus m.
Ophthalmic n. (V1) Maxillary n. (V2) Mandibular n. (V3)
Optic canal (II) Sup. orbital fissure (III, IV, VI, V1) F. rotundum (V2)
What might be the consequence • if the infectious material invaded • the internal carotid artery within • the sinus?
Mid. cerebral a. Ant. cerebral a. Cavernous sinus containing ICA
Ant. cerebral a. Ant. communicating a. ICA Mid. cerebral a. Post. communicating a. Post. cerebral a. Basilar a. Vertebral a.
Superficial middle cerebral v.
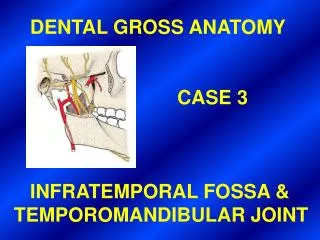
9. Explain how osteomyelitis (inflamation of the bone and marrow) of the upper or lower jaw following tooth extraction could lead to infectious cavernous sinus thrombosis. (Hint: What important venous structure lies in the infratemporal fossa?)
Emissary v. connecting w/ cavernous sinus via f. ovale Post. sup. alveolar v. Pterygoid plexus of vv. Inf. alveolar v.
Additional Note Infectious cavernous sinus thrombosis was almost invariably fatal prior to the advent of antibiotics. In this era of intensive antibiotic treatment the condition is not as common as it used to be but the prognosis, should one contract it, is grim — 80% mortality and in the survivors 75% after effects, mainly involving eye muscles and changes in visual acuity.