Download
1 / 73
770 likes | 1.12k Views
A Case of Cerebral Venous Sinus Thrombosis (CVST). McGill Stroke Rounds Chenjie Xia (R2) Wednesday, April 28 th , 2010. Outline. Case introduction Overview of CVST Anticoagulation in CVST Role of steroids in CVST Management of seizures in CVST. Outline. Case introduction

E N D
A Case of Cerebral Venous Sinus Thrombosis (CVST) McGill Stroke Rounds Chenjie Xia (R2) Wednesday, April 28th, 2010
Outline • Case introduction • Overview of CVST • Anticoagulation in CVST • Role of steroids in CVST • Management of seizures in CVST
Outline • Case introduction • Overview of CVST • Anticoagulation in CVST • Role of steroids in CVST • Management of seizures in CVST
Mr. GC • ID: • 38M, right handed • originally from Australia, now works as oceanography researcher in Honolulu • PMHx: • Nil • no known previous clotting d/o • FMHx: • DVT in maternal grand-mother • Meds: • Nil at home • Habits: • non-smoker, occasional EtOH
Mr. GC • HPI: • July 19th2009: flight of 10hrs on from Honolulu to Montreal for oceanography conference • Drank ½ litre of wine prior to flight (slightly unusual consumption) • Slight HA and nausea for 3 days PTA • PTA: no fever or other malaise, no focal neurological signs (aphasia, visual changes, motor or sensory changes), no recent infection/fever/weight loss or other constitutional symptoms
Mr. GC • HPI (continued): • July 20th: brought to MGH by EMS with sudden onset GTC seizure lasting 1 minute at the conference • Repeated GTC seizure while in the MGH ER • Course at MGH: • O/E : expressive aphasia, Rt hemiplegia • CT head: left frontal 24 x 35mm ICH with edema, mild mass effect, no midline shift • Given Dilantin load and Ativan PRN for seizure control • Transferred to MNH NICU
Mr. GC • O/E at MNH (July 21st): • Neck supple, afebrile, vitals normal • Mental status • Severe expressive aphasia (answers mostly limited to yes/no, < 4 words sentences, good repetition, able to read without difficulty) • Follows first-second order command • CNs: • pupils b/l reactive 4mm, fundi right normal, left not well seen, VFs normal • right facial droop (UMN distribution) • rest of the CNs unremarkable
Mr. GC • O/E at MNH (July 21st): • Motor: • toneRight UE and b/l LEs • Dense right hemiplegia, normal left side strength • reflexes (3+ at right arm and bilateral legs, right ankle 4-5 bts clonus, equivocal toes) • Sensory exam (normal to LT, T and vibration) • Cerebellar: normal left UE FTN and RAM
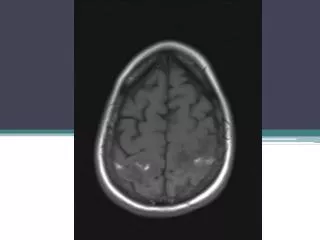
Mr. GC CT head (July 20th) MRI T2 FLAIR (July 21st)
Mr. GC MRV (July 20th)
Mr. GC • Imaging: • CT head: • left frontal hematoma at high convexity with +++ edema • Thickening / hyperdensity of SSS, suspicion of venous thrombosis • MRI/MRV: • left frontal intraparenchymal bleed (with focal mass effect and effacement of subarachnoid spaces, minimal compression of the left lateral ventricle) • Signal void involving the anterior and middle portions of the SSS, highly compatible with sinus thrombosis • MRV reveals thrombosis of anterior and mid portion of the SSS
Outline • Case introduction • Overview of CVST • Anticoagulation in CVST • Role of steroids in CVST • Management of seizures in CVST
CVST - Epidemiology • 3-4 cases / million in adults; 7 cases / million in children; 5-8 cases / year in a tertiary care centre • 75% of adults are women, M:F = 1.5/5 • Peak incidence in third decade in adults • Highly variable symptoms and clinical course • > 80% have good neurologic outcome
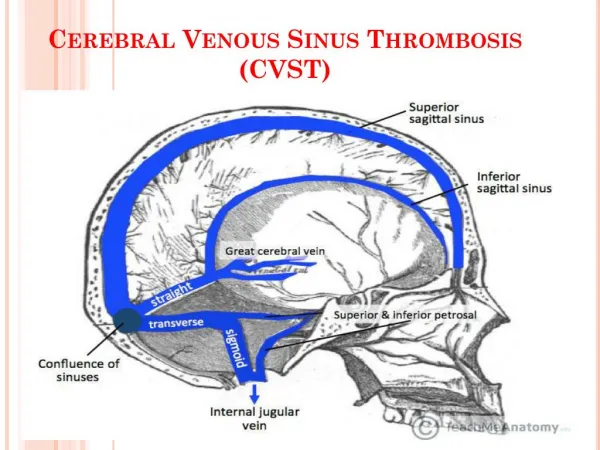
CVST - Pathogenesis • Mechanisms: 1) Thombosis of cerebral veins • localized edema and venous infarction • combination of cytotoxic and vasogenic edema 2) Thrombosis of major venous sinuses • venous pressure and impaired CSF absorption intracranial hypertension • No pressure between subarachnoid spaces at surface of the brain and ventricles no hydrocephalus
CVST - Pathogenesis Jan Stam. Thrombosis of the cerebral veins and sinuses. The New England Journal of Medicine, April 28, 2005.
CVST – Causes and Risk Factors • Prothrombotic risk factor (genetic or acquired) • Dehydration • Head trauma • Neurosurgical procedures • Obstetrical delivery (12 / 100 000 deliveries) • OCPs • LP • Infections (otitis, mastoiditis, paranasal sinusitis, orbit or facial infections) • 43% of patients will have > 1 RF
CVST – Clinical Manifestations • Headache • most common, 90% of all cases • Focal neurological signs • motor, sensory deficits, aphasia, hemianopsia • Seizures • Behavioural problems • Amnesia, personality change • Thalamic lesions • Stupor or coma • from herniation, seizures, bilateral thalamic involvement • Isolated intracranial hypertension • 20-40% • Headache, n/v, papilledema, diplopia
CVST - Diagnosis • Delay from onset of Sx to Dx: • Average = 7 days • Diagnostic modalities: • MRI, MRV • best tools for Dx and F/u • CT, CTV • Can be used for Dx • limited for F/u (radiation, contrast) • Conventional angio • Previous gold standard • May be useful in cases of isolated thrombosis of cortical veins without sinus thrombosis
CVST - Treatment • Acute management of patients with impaired LOC • Role of anticoagulation (controversial…) • Role of thrombolysis • Control of seizures • Chronic intracranial hypertension management
Mr. GC • Course of hospitalization: • Initial decision made not to A/C for now given hemorrhage • Plan repeat MRI/MRV in 1 week, then reconsider A/C • 1 week later…
Mr. GC CT head (July 27th) MRI T2 FLAIR (July 27th)
Mr. GC • Imaging: • CT head: • Evidence of edema causing significant mass effect with right midline deviation of 6 mm. • The left lateral ventricle is compressed • no interval change in the size of left frontal hemorrhage. • more conspicuously seen edema and mass effect • MRI/MRV: • increased surrounding edema, midline shift to the right • further compression of the lateral ventricle • no evidence of recent hemorrhage • Again demonstrated is hyperintensity in the two anterior thirds of the SSS in keeping with thrombosis • MRV does not demonstrate any significant change
Mr. GC • July 27: • Clinical progress • Increasing ease in word-finding • Start to form short complete sentences • Increasing strength of right hemibody • Again, decision made not to A/C due to clinical stability / improvement. • Plan: repeat imaging in one week and then reevaluate need for A/C…
Outline • Case introduction • Overview of CVST • Anticoagulation in CVST • Role of steroids in CVST • Management of seizures in CVST
A/C in CVST – The Controversy • Not a new problem… • Hugo Krayenbuhl, Swiss neurosurgeon (1902-1985) said in his 1966 summary of 73 patients with CVST: “We have no proof that cerebral hemorrhages occur more often and are more severe in anticoagulated cases. The group without any treatment has the highest mortality.” http://www.societyns.org/society/bio.aspx?MemberID=14400
A/C in CVST – The Controversy • Rationale FOR use of A/C in CVST • Avoid thrombus extension • Favour spontaneous thrombus resolution • Prevent pulmonary embolism • Rationale AGAINSTuse A/C in CVST • Promote or worsen ICH • Promote extracerebral bleeding complications
A/C in CVST – The Evidence • Einhaupl et al. Lancet 1991 2 groups of 10 patients each average delay to treatment 10 days
A/C in CVST – The Evidence 2) De Bruijn et al. Stroke 1999 2 groups of 30 patients each average delay to treatment 4 weeks
A/C in CVST – The Evidence • Cochrane review: primary outcome (death) Stam et al. Anticoagulation for cerebral sinus thrombosis (Review). The Cochrane Collaboration, 2008
A/C in CVST – The Evidence • Cochrane review: primary outcome (death or dependency) Stam et al. Anticoagulation for cerebral sinus thrombosis (Review). The Cochrane Collaboration, 2008
A/C in CVST – The Evidence • Cochrane review: secondary outcome (new or recurrent intracerebral hemorrhage) CI = 0-9% Stam et al. Anticoagulation for cerebral sinus thrombosis (Review). The Cochrane Collaboration, 2008
A/C in CVST – The Evidence • Cochrane review: secondary outcome (extracerebral hemorrhage) Stam et al. Anticoagulation for cerebral sinus thrombosis (Review). The Cochrane Collaboration, 2008
A/C in CVST – The Evidence • Is A/C safe in patients with CVST complicated by hemorrhage? • Fink et al. Neurology, 2001 • Starting points: • Increasing evidence heparin is safe for CVST with hemorrhage • Uncertainties about safety of heparin in presence of large hemorrhages
A/C in CVST – The Evidence • Fink et al. Neurology, 2001 • Findings • 25 cases of CVT: 14 with ICH, 9 of which > 4cm3 • 7/9 ICH patients treated with heparin: • 0/7 had significant recurrent ICH or clinical deterioration • 3/9 patients were initially not treated with heparin: • 2/3 had recurrent ICH in different vascular territory (1 eventually died) • 1/3 was subsequently treated with heparin and clinical deficits resolved completed
A/C in CVST – The Evidence • Fink et al. Neurology, 2001 • Conclusions • Heparin is safe in CVT with large hemorrhage • De novo recurrent ICH (i.e. in different vascular territory) occurred only in those not treated with heparin & subsequent improvement occurred only if heparin was instituted • Limitations of study: retrospective, non-randomized
A/C in CVST – The Evidence • ISCVT (International Study on Cerebral Vein and Dural Sinus Thrombosis): • prospective multinational observational study involving 89 centres in 21 countries • 624 consecutive adult patients with symptomatic CVT (recruited from May 1998 to May 2001) • Dx confirmed by angio, CTV, MRV, surgery or autopsy • Choice of treatment left up to treating physician (i.e. no randomization)
A/C in CVST – The Evidence • ISCVT (cont’d): • 83% of patients received UFH or LMWH in the acute phase reflects general consensus among neurologists re: A/C in acute CVST? • Safety of heparin • ¾ with early ICH were treated with therapeutic heparin (rate similar to non-ICH patients) • Heparin associated with better outcome (all delayed ICH patients who had good outcome were treated with heparin) • Limitation: use of heparin was not randomized nor blinded
A/C in CVST – The Evidence Girot et al. Predictors of outcome in patients with cerebral venous thrombosis and intracerebral hemorrhage. Stroke, 2007.
A/C in CVST – The Conclusion • Cochrane review 2008: • “A/C treatment for CSVT appeared to be safe and was associated with potentially important reduction in risk of death or dependency which did not reach statistical significance” • Future RCTs with A/C vs placebo may be difficult to initiate due to lack of equipoise • May still be reasonable to collect more data from cohort series or case-control studies to estimate A/C-related risk
A/C in CVST – The Conclusion • EFNS (European Federation of Neurological Societies) 2010 guidelines: • Level B recommendation for use of A/C • Concomitant ICH is not a contraindication • LMWH may be preferable • Studies with DVT shows risk for extracerebral bleed with LMWH compared to UFH
A/C in CVST – The Consensus? • Letters to the editor, Archives of Neurology 2008: • AGAINST (Walsay et al.) • Good natural history without treatment • No statistically significant from RCTs • Physicians choose to A/C because “they find it extremely difficult to do nothing.” • AMBIVALENT (Roach) • Data favoring A/C is suggestive, but not compelling • More RCTs needed? • FOR (Stam) • A/C corrects underlying mechanism of hemorrhage: thrombosis capillary pressure local cerebral edema petechial hemorrhage • Cannot ignore the ARR of 13% found in RCT (p = 0.08) from meta-analysis
A/C in CVST – Long-term • Long-term oral anticoagulation • Recanalization • Occurs within first 4 months irrespective of further OAT • Even if incomplete or no recanalization, CVST recurrence rare • CVST Recurrence • Risk may be lower than in extracerebral VTE • ISCVT: during 16 months f/u 2.2% recurrence • Despite above… • Most still offer long-term OAT • ISCVT: at 6 months, 80% of patients were on OAT; median time on OAT = 7.7 months
A/C in CVST – Long-term • EFNS guidelines • Optimal duration unclear, target INR 2-3
A/C in CVST – Final Words • Still the same problem: • Hugo Krayenbuhl (1966): “We have no proof that cerebral hemorrhages occur more often and are more severe in anticoagulated cases. The group without any treatment has the highest mortality.”
Mr. GC • July 27: • Clinical progress • Increasing ease in word-finding • Start to form short complete sentences • Increasing strength of right hemibody • Again, decision made not to A/C due to clinical stability / improvement… • Plan: repeat imaging in one week and then reevaluate need for A/C
Mr. GC CT head (August 4th)
Mr. GC • Imaging of August 4th: • size and density of the left frontal hematoma have diminished significantly • surrounding vasogenic edema has diminished slightly • left frontal horn is starting to reexpand • midline shift has improved