Download
1 / 29
300 likes | 515 Views
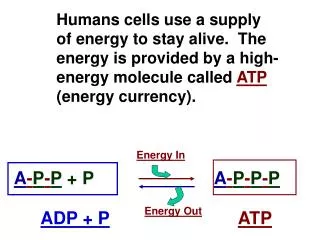
Sabrina Ermayanti. KEGANASAN P LEURA. Bagian Pulmonologi dan Kedokteran Respirasi FK Unand. Structure of the Thoracic Cavity. Pleural Anatomy. Lungs are surrounded by thin tissue cal l ed the pleura , a continuous membrane that folds over itself Parietal pleura lines the chest wall

E N D
Sabrina Ermayanti KEGANASAN PLEURA BagianPulmonologidanKedokteranRespirasi FK Unand
Pleural Anatomy • Lungs are surrounded by thin tissue calledthe pleura, a continuous membrane that folds over itself • Parietal pleura lines the chest wall • Visceral pleura covers the lung (sometimes called the pulmonary pleura)
Schematic diagram of pleural anatomy; s.c.=systemic capillary; p.c.=pulmonary capillary
SelMesothelial • selapisselmesothelial • pavement-like cells • melapisipermukaan pleura • sel yang aktif, sensitif & responsif • terhadapberbagairangsangan • dinamik
SelMesothelial Fungsi : • transportasidanpergerakancairan danpartikel • migrasileukosit responinflamasi • sintesissitokin, fcpertumbuhan & matriksekstraseluler • melepaskanfcutkmerangsang deposisidanpembersihan fibrin dan antigen
Cairan Pleura Volume: Normal sedikit (+) Noppen et al. 8,4 ± 4,3 ml. Terdiridari: protein (tu. albumin,globulin, and fibrinogen) sel (tu. Selmesothelial , monocytes, and lymphocytes) Pd manusia 75% macrophages 25% lymphocytes < 2% mesothelial cels, neutrophils and eosinophils
Neoplasma Pleura • Primer • benign (jarang) • Lipoma • Fibroma • Endotheliomas • Angiomas • Cysts • malignant mesothelioma • Secondary • >> adenocarcinomaparu, GIT, ovarium
Insiden • penggunaanasbestos stlh PD -2 [McDonald 1987] • Negara Industri : 2 per satujuta♀ 10 - 30 per satujuta♂ ♂ = 10 x ♀ • Resiko >> daerahgalangankapal • 5-7% dariorang yang terpapar asbestos • 50% tidakadariwayatterpapar asbestos
Insiden • Occupational Exposureto Asbestos • AS >> th 2004 = 2.300 paparan > th 30-60 • Eropa Barat >> th 2018 = 9.000 > th 70 • Laten period 20 - 40 tahun • Paparan dg gedungygdiisolasi dg asbestos sangatjarang [Hughes et al. 1986; Lilienfield 1991
Gejala Umur 40 – 70 th 2/3 kasus Riwayatterpapar asbestos 20 thsebelumnya ataulebih Nyeri dada nonpleuritik menjalarke abdomen atas / lengan Sesaknafas >> BB , batukkeringdandyspnea bbrppasien demamtdktinggi ManifestasiKlinis
Tanda Tanda –tandaefusi pleura I = cembung, pergerakantertinggal Pl = fremitus < Pk = redup – pekak A = Suaranafas -sp (-) Clubbing finger Atrial fibrillation ManifestasiKlinis
PemeriksaanPenunjang • Ro thoraks • 70-95% efusi pleura • efusimasif • 50% hemitoraks • tidakjelasgambaran • tumor pleura
PemeriksaanPenunjang • CT Scan toraks • pleura menebal • terutama pleura • mediastinum • irreguler • volume hemitoraks yang • kenabervariasi • 30-42% mengecil
PemeriksaanPenunjang • Sitologicairan pleura • 3 Tipesel • Epithelial Type : 50 % of cases • most often confused with adenocarcinoma • Mesenchymal Type : 16 % of cases • Mixed Type : 34 % of cases
PemeriksaanPenunjang • Sitologicairan pleura
PemeriksaanPenunjang • MRI • Bronkoskopi • Biopsi pleura • Tertutup • Terbuka • VATS
Diagnosis (2) • Cardinal Characteristics [Boutin 1998] • Age between 55 - 65 • Previous occupational exposure to asbestos • Pleural Effusion • C.T. / MRI (with nodular lesions of the parietal pleura)
Staging I Confined to ipsilateral pleura II Involves chest wall, mediastinum, pericardium or contralateral pleura III Involves both thorax and abdomen or lymph nodes outside thorax IV Distant metastasis
Treatment There is no single treatment which has proven effective... Surgery Radiation Chemotherapy Immunotherapy Gene Therapy
Tumor metastaseke pleura • Insiden : penyebabefusi pleura eksudat no 2 setelah parapneumoniefusi • Tumor primer • kankerparu • kankerpayudara 75% • limfoma • lain2 Ca ovarium, sarcoma, Ca lambung, Ca kolon, Ca pankreas, Ca buli2 dll
ManifestasiKlinis • Gejaladantandaefusi pleura • Gejaladantanda tumor primer
PemeriksaanPenunjang Ro toraks CT Scan toraks Sitologicairan pleura Biopsi pleura
PemeriksaanPenunjang • Tes Immunochemical • Adenoca CEA; MOC-3,1; B72,3; Ber-EP4 & BG-8 • Tumor marker pd cairan pleura • CEA; CYFRA21-1; SCC antigen;SSEA-1
Penatalaksanaan • Punksicairan pleura • Kemoterapisistemik • Radioterapi • Radiasimediastinal • Pleurodesis • Indwelling Pleural catheter • Pleuro-peritoneal shunt