Download
1 / 19
190 likes | 228 Views
Learn about acute and chronic kidney disease, dialysis options, essential lab values, diet recommendations, medications, and challenges faced by ESRD patients. Maximize patient care with proper assessment, planning, education, and monitoring techniques.

E N D
Nutrition and Kidneys MNT Approaches to Acute and Chronic Kidney Disease
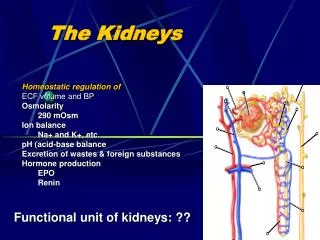
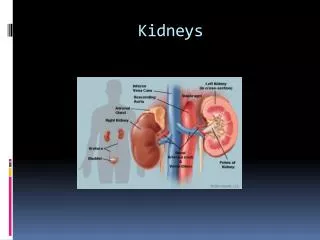
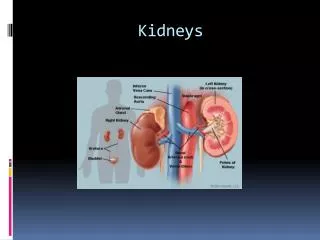
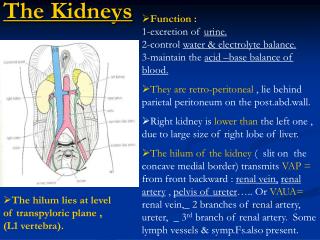
What happens when Kidneys shut down? • Waste products • Water/fluids • Parathyroid • Electrolyte balance • The diet of patients with compromised kidney functioncorrects the chemical imbalances
Key Labs to Watch • BUN/Creatinine • K • Phos • Albumin • Hgb, Hct • Calcium • Body weight changes
Acute Renal Failure • Short term kidney failure • See rapid change in chemistry, water retention • Cause: infection or trauma • Diet Rx: support underlying disease process, keep comfortable, monitor for fluid buildup
Chronic Renal Failure • Slow to occur – gradual onset • Causes: uncontrolled HTN, DM, CA, Lupus, trauma • Symptoms – yellowing of skin, retention of water, weight loss, appetite loss, “don’t feel good” usually brings to Dr OR product of long term monitoring
Diet Rx for CRF (predialysis) • To retard kidney destruction, limit protein to .08g/kg/day. • Sometimes losing too much water and electrolytes – base this on the chemistries
Going on Dialysis Types of treatments • Hemodialysis • In Center • Home • Peritoneal • Continuous (CAPD) • Intermittent (IPD) • Continuous Cyclic (CCPD) • Transplant
Diet for Hemodialysis • 1 gm protein per kg body weight • 2 gm K • 2 gm Na • Limited phosphorus • 1500 cc fluid q d • Kcalories to meet need or control blood glucose
Typical Lab Panels • BUN – look for up to 100 pretx • K - < 6.0 • P - < 6.0 • Alb - > 3.0 • Wt changes – 2-3 kg • Monitor weight trend by post tx when they are “dry”
Medications (lots) • Calcium supplement (phosphate binder • Multivitamin • Iron supplement or antianemics • Antihypertensives (usually) • Control of other conditions eg, CA tx, oral agents, CVD
Pros/Cons of Hemodialysis • Someone else controls tx • Scheduled • Control over cleansing of blood • In center attention and often • But • Fluid buildup • Constant control of external chemicals to prevent buildup • BP drops • Access infections
Peritoneal Dialysis • Continuous exchanges of sugar fluids to remove waste • Goods: feel better, better clearance of chemistries, less restrictive diet • Bads: requires independence, weight gain, difficult protein balance, more difficult to control BGL, high susceptibility to infection of access
Diet Rx for Peritoneal Dialysis • High protein – 2 gm/kg body weight • Calorie controlled • Balanced nutrients • Phosphorus restriction
Meds for Peritoneal patients • Multivitamin • antianemics • Support meds for underlying conditions
Labs for Peritoneal patients • BUN – 40-50 • Albumin > 3.0 • Phos < 6.0 Spend lots of time counseling on balance between adequate protein and just enough kcalories to control weight (additional kcals from dialysate fluid)
Transplant – the end of Kidney Disease? • Symptoms and ramifications of ESRD subside • High doses of antirejection drugs result in weight gain (round face) • Also they feel better, and eat more • Diet Rx: kcalorie controlled, balanced (avoid weird stuff)
Issues with ESRD patients • Noncompliance • Denial • Lose hope • More and more elderly • Family control of diet
What you do when you work with a patient with renal disease • Assess: no question is high acuity level, start as you would anyone else with calculating nutrient needs and adjustment • Plan: continous, they are going to be with you awhile • Educate: ongoing, sometimes fruitless, develop a trust level with your patients • Monitor: look for trends and real changes