Addressing Mental Health Needs for Youth through Community-Based Interventions in Thurston and Mason
An annual assessment in Thurston and Mason counties revealed that 1,800 youths up to age 20 are engaged in the public mental health system. Notably, 9% of these youth incur over half of the mental health expenditures, many being involved in multiple systems. The assessment identified access to services as a primary barrier. This led to the selection of Multisystemic Therapy (MST) as a priority intervention. The program aims to enhance service delivery through a community-based model, ensuring that evidence-based practices effectively meet the complex needs of multi-system involved youth.

Addressing Mental Health Needs for Youth through Community-Based Interventions in Thurston and Mason
E N D
Presentation Transcript
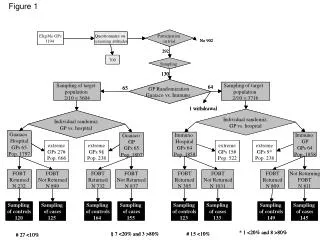
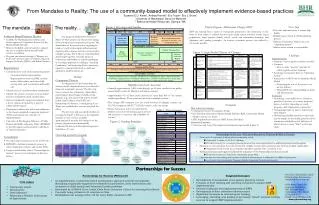
Highlights from Needs Assessment • Annually, approximately 1,800 youth through age 20 were enrolled in the public mental health system in Thurston and Mason counties. • Approximately 9% of these youth account for more than half of the mental health expenditures. These youth are involved in multiple systems. • The average MH treatment cost for youth involved in multiple systems was $19,742, compared with $1,773-$3,032/youth in only one system. Figure 1. Key steps and timeline • Needs Assessment survey revealed that the primary reason for their being a gap in services and resources is “access to and availability of services.” From Mandates to Reality: The use of a community-based model to effectively implement evidence-based practices Suzanne E.U. Kerns1, Andrea Parrish2, Eric Trupin1, Eric J. Bruns1 1 University of Washington School of Medicine 2 Behavioral Health Resources, Olympia, WA Next Steps - Fine-tune implementation to ensure high fidelity - Redeploying of funds for Tribal planning process - Enhance Community Team’s role as an “Operating System” - Address issues related to sustainability The mandate…… The reality… Priority Program : Multisystemic Therapy (MST) MST was selected from a menu of 8 programs presented to the community on the basis of their ability to address known needs (multi-system involved youth), target populations, target impacts (family, school, youth, and community domains), and alignment with guiding principles. An iterative consensus process was utilized to choose the practice. • Evidence-Based Practices Proviso • In 2006, the Washington State House and Senate approved a Legislative Proviso for the Mental Health Division • Mission: Establish a pilot program to expand the use of evidence-based mental health services to children • Program site selected through a “Request for Proposals” process, open to counties, Regional Support Networks (RSNs), and Indian Nations • Requirements • Commitment to work with community partners • Consumer/family representatives • Representatives from local MH, juvenile justice, child welfare, and other child-serving areas such as education and health care • Identify areas of need from these stakeholders • Identify the service or services to be provided based on community needs and resources • Select an empirically supported treatment from a list of options developed by a panel of subject matter experts • Participate in efforts that will ensure adherence to the chosen empirically supported treatment (ESTs) and evaluate the outcomes of implementation • University of Washington, Division of Public Behavioral Health and Justice Policy (DPBHJP) to provide support and assistance in all phases of the pilot program • Consultation • Provided under contract as part of the Proviso • DPBHJP to facilitate community process to select, implement, evaluate, and sustain ESTs • Largely modeled after Ohio’s “Partnerships for Success” process (see description in blue box below) The proposal submitted by Thurston-Mason (T-M) Counties was chosen for funding from among several competitive proposals. The initial frame of the proposal was targeting the needs of youth with complex behavioral and mental health concerns and who are involved in multiple systems. The T-M core team identified and brought together a broader group of community stakeholders to actively participate in a strategic approach to building a “Learning Community” and increasing their community’s capacity to respond effectively to child and adolescent problem behaviors. Method Community Process An adaptation of the Partnerships for Success model (described below) was utilized to frame the community process. The first step was to convene key community stakeholders, representing a broad range of child-serving agencies (e.g., schools, juvenile justice, mental health, child welfare), about ESTs and Partnerships for Success. A small group (Core Team) was established to oversee and guide the effort. The key steps and associated timeline are presented in Figure 1. Because of the legislative mandate to have services available approximately 6 months after initiation of the project, the process was dramatically condensed from a more ideal planning process timeframe of 1 year. Choosing a priority program Figure 3. Logic Model (Theory of Change) • Challenges • Implementation • Timeline – had to greatly condense activities • Contracts • How to make “process” activities fit within typical contract language • Sustaining Community Team as “Operating System” • Intersection of MST with Community Mental Health • Navigating the role of the purveyor in service delivery • Fitting MST into existing billing structure and infrastructure • Evaluation • Identifying a reasonable set of evaluation priorities in the face of so many proposed layers of activity (impacting on youth, program, staff, stakeholder, community) • Anticipating length of time to realize long-term impacts • Determining feasible methods to rigorously test the impact of the model, given the above complexity and likelihood of diffusion of effects across so many "links" in the logic chain Inputs Activities Outcomes Long-Term Impacts Proviso funding Regional Support Network Mental Health Division • Development of an EBP workgroup (community team) • Participate in Partnerships for Success collaborative process • Review data on community resources and child well-being indices • Review implementation progress and outcome data • Participate in development of a sustainability plan • Cross agency collaboration and fiscal blending • Improvements in collaborative planning between community & state partners • Strategic plan • Sustainability plan • Ability to serve children and adolescents within their own communities • Expanded services and supports • Improved access to services • Cost savings System Level + Bridge Level Community & Tribal stakeholders Behavioral Health Resources In-kind resources University of Washington Project workgroups • Identification of Core Team members to provide project oversight and coordination • Collect data on needs and resources from a community perspective • Identify gaps in services and service priorities (i.e., targeted impacts and target population) • Identify empirically-supported treatment/s • Develop an implementation plan in alignment with guiding principles • Utilize data (e.g., process evaluation) to make decisions • Conduct planning process with Tribal communities • Community able to respond to identified needs • Coordinated services for youth involved in multiple systems • Implementation • Enhanced collaboration with UW • Reduced disparities for minority youth (incl. Tribal youth) • Enhanced ability to receive funding to address children’s mental health issues • Ability to quickly mobilize around additional opportunities or problem-solving needs + Practice Level Multisystemic Therapy intervention team Administrative supports • Mental health Sx and functional impairment • Out-of-home placements • Academic, social, and emotional health • Recidivism • Family functioning • Improved social supports for families in the community • More skilled provider staff • Youth prevented from deeper penetration in systems • Articulate goals and guiding principles • Implement MST with fidelity • Participate in outcome evaluation + • Evaluation • Data collection strategies: • Community Surveys (Community Team) • Key Informant Interviews (Mental Health Division, RSN, Community Mental Health Center, Core Team) • MST Implementation Surveys (MST Service Providers) • Measured Outcomes: • Outcomes and Long-Term Impacts articulated in logic model (Figure 3) Table 1. Target Impacts Figure 2. Guiding Principles • Partnerships for Success – Perceived Benefits for Thurston & Mason Counties • Promotion of systematic thinking about community needs • Generated “outside of the box” thinking • Provided context for a strategic planning process that can be generalized to additional projects and programs • Initiation of a new program for youth involved in multiple systems with community buy-in from multiple stakeholders • Organized system to pull key community members together with a common focus • Technical assistance and support facilitated the utilization of the Partnerships for Success model • Promoted context for University-community partnership • Opportunities for networking and contacts resulted in infrastructure for adoption of additional programs • e.g., Foster Care Assessment Program; Family Integrated Transitions program Partnerships for Success For more information about Partnerships for Success, contact Melissa Ross at: Ohio State Center for Learning Excellence 807 Kinnear Road, Columbus, Ohio 43212 (614) 292-0175 Email: ross.565@osu.edu www.pfsacademy.org • Targeted Outcomes • Development of sustainable cross-agency planning entities • Creation of local training and coaching consortia to support EBP implementation • Increased adoption and implementation of EBPs • Development of data collection infrastructures • Significant increases in external grant funding • Leveraging, blending, and pooling of previously “siloed” internal funding sources to support EBP implementation • Partnerships for Success (PfS) model • A comprehensive, community-based participatory approach towards strategically identifying empirically-supported treatments for prevention, early intervention and treatment of child mental and behavioral health problems • Developed by Al Neff & Dave Julian (Ohio State University Center for Learning Excellence) • Currently being utilized in 44 counties in Ohio • Established cost savings of $11.52 for every dollar invested in PfS • Core values • Community based • Participatory • Data-informed • Balancing a Holistic Continuum of Approaches