Download
1 / 66
740 likes | 1.32k Views
Acute & Chronic Pancreatitis. Armed Forces Academy of Medical Sciences. Alexander the Great in 3rd century B.C. Age 33 returned to Babylon from Persian victories Celebrated with his generals and “ETOH flowed freely” Next day he was seized with abdominal pain

E N D
Acute & Chronic Pancreatitis Armed Forces Academy of Medical Sciences
Alexander the Great in 3rd century B.C. • Age 33 returned to Babylon from Persian victories • Celebrated with his generals and “ETOH flowed freely” • Next day he was seized with abdominal pain • Tx: immersion in waters of Euphrates • 1st record of chronic pancreatitis in 1787 • affluent, social man seized with diabetes • autopsy showed pancreas filled with stones
AP - Introduction • Incidence 1-5/10,000/yr • Overall Mortality 2-5% • 180,000 Hospitalizations/year US • 2300 Deaths/year US
AP • 80% mild(interstitial or edematous) • 20% severe (necrotizing) • 40-70% severe cases infected • Mortality infected cases 27-45%
AP - Pathophysiology • Autodigestion - primarily due to activation of trypsin • Pancreatic proteases (trypsin, chymotrypsin, elastase, carboxypeptidase and phospholipase A) • secreted as proenzymes • Trypsin is central to this activation and is activated by duodenal brush-border enteropeptidase
AP - Pathophysiology Resolution
Acute severe upper abdominal pain, 95% Back radiation, 50% Nausea/Vomiting lasting hours Abdominal tenderness, guarding, peritoneal signs Fever Tachycardia Leukocytosis AP - Clinical Presentation
AP - Clinical Presentation • Severe pancreatitis • hypotension (fluid sequestration) • SIRS • Cullen sign (periumbilical purpura) • Grey Turner sign (left flank purpura) • hemorrhagic pancreatitis • retroperitoneal hemorrhage
AP - Differential Diagnosis • Mesenteric ischemia/infarction • Perforated GU/DU • Intestinal obstruction • Biliary colic • Inferior wall MI • Ectopic pregnancy
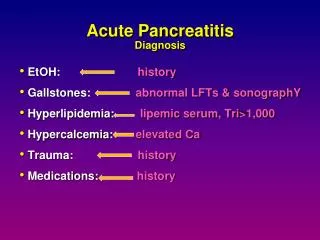
AP - Diagnosis • THIS IS A CLINICAL DIAGNOSIS • History: Boring epigastric/LUQ • Physical: tenderness, guarding • Labs: CBC, Chemistry, LFT’s, Amylase or Lipase • Plain X-rays: r/o perforated viscous • US: gallstones/ductal dilation/cholecystitis • CT: ONLY to evaluate for severity and complications (normal in 15-30% mild cases) • MRCP: Elevated ALT/AST/Bili/AP and no stones seen on RUQ US.
Amylase/Lipase - Dx • Amylase • 3x ULN • 1/2 life 2 h • Increased values secondary to increased release and decreased clearance • Rapid clearance w/i 24h • Biliary > 1000 • Alcohol < 500
Lipase - Dx • Lipase • Test of choice for most clinicians • 3x ULN • Better sensitivity/specificity than amylase • Useful early as rise parallels amylase • Useful in delayed presentations secondary to slow clearance • Only from pancreatic origin (ddx includes chronic pancreatitis, pseudocyst, malignancy)
Acute Pancreatitis - Dx • Height of amylase and lipase DOES NOT correlate with severity • Once Dx is made, daily measurement of serum amylase has little if any value in assessing the clinical progress of the patient or ultimate prognosis
AP - Severity Ranson’s Criteria Risk Factors Mortality <2 <1 % 3-4 16 % 5-6 40% 7-8 ~100%
AP - Severity • APACHE-II Severity of Disease • A. Acute physiology Score • B. Age Points • C. Chronic health points • *** Score <8 ---> good prognosis • Various other similar scores including APACHE III
AP - Severity Organ failure is the most important indicator of severity of AP • SIRS • Renal Failure, Cr > 2 mg/dl • GI Bleeding, >500 ml/24 h
AP - Treatment • Mild AP • Fluid resuscitation • Careful monitoring • Largely supportive • CT scan generally not helpful in management of mild AP • Most mild AP have interstitial dz
AP - Treatment • Severe AP • Contrast CT recommended at some point beyond the first 3 days in severe AP to r/o necrotizing pancreatitis/infection • o/w early CT has not been validated, risk controversial wrt increased microvascular ischemia
AP - Treatment • Important Concepts in Managing AP • Recognition of clinically severe AP • Scoring system • Identification of stone disease • ICU management for severe AP • Prompt diagnosis of infected necrosis • Debridement of infected necrosis
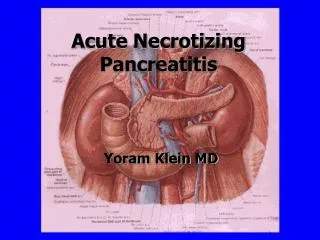
Definition of Pancreatic Necrosis Diffuse or focal area(s) of non-viable pancreatic parenchyma usually associated with pancreatic fat necrosis. May be sterile or infected.
Dx of Infected pancreatic necrosis • Difficult to make clinical diagnosis • fever, leukocytosis, and unresolved organ failure • severe pain seen with both sterile and infected necrosis • CT/US guided FNA procedure of choice • safe • accurate • Gram Stain • 96% sensitivity, 99% specificity
Prophylactic Abx • Infection of pancreatic necrosis is primary cause of mortality after 7 days • Prophylactic abx • Most recent Cochrane review (2003) • Decreased mortality (OR 0.32) • Decreased pancreatic sepsis (OR 0.52) • Best studies showed least benefit
Prophylactic Abx • On sub-group analysis, imipenem was only abx to show benefit • However, recent RCT showed no benefit with meropenem • No evidence for risk of fungal superinfection • Guidelines have varying opinions • Clearly should only be used in high-risk patients (ie >30% necrosis) for no more than 14 days
Nutritional Support • 3 meta-analyses favor enteral over parenteral nutrition • Less sepsis, lower inflammatory markers, much less expensive • Only relevant in severe pancreatitis • Jejunal feeding best-studied, not most practical • Ileus is not a contraindication • Start 3-5 days into course, benefit compared to TPN disappears if started after 7 days • TPN is better than no nutrition
Chronic Pancreatitis • Remains a major source of morbidity in US • Admissions average 10 days • Frequent narcotic need • Increased risk of pancreatic ca • Dx usually made after dz is well established • Mortality from complications: 25% at 5 years
Chronic Pancreatitis “Continuing inflammatory disease of the pancreas characterized by irreversible morphologic changes that typically cause pain and/or permanent loss of function” • Gastroenterology 2001;120
Etiologies of chronic pancreatitis Cystic fibrosis Hereditary pancreatitis Hypertriglyceridemia Autoimmune Fibrocalcific Other Alcoholic Idiopathic