Download
1 / 31
320 likes | 466 Views
Peripheral Arterial Disease of the Lower Limb Diagnosis and Medical therapy. Marco Alemán, MD Division of General Medicine University of North Carolina at Chapel Hill July 13, 2010. Disclosures. NO commercial affiliations NO commercial support. Agenda. Definition of PAD Epidemiology

E N D
Peripheral Arterial Disease of the Lower LimbDiagnosis and Medical therapy Marco Alemán, MD Division of General Medicine University of North Carolina at Chapel Hill July 13, 2010
Disclosures • NO commercial affiliations • NO commercial support
Agenda • Definition of PAD • Epidemiology • Diagnosis • Medical Therapy
Case 1 • 64 yo man with tobacco abuse, high cholesterol presents with 6 month history of left leg aching when walking.
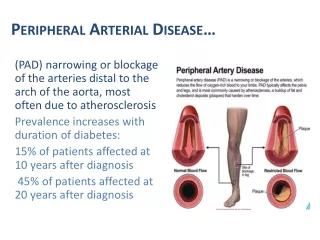
PAD Definition Pain in a functional muscle unit • which is reproduced by exercise • causing the patient to stop walking • promptly relieved by rest (less than 10 minutes)
PAD Epidemiology • PAD prevalence 2- 12% • Cardiovascular Health Study of community patients ≥ 65 year of age • Using ABI: 12% prevalence • Men who have heart disease or stroke • 30% prevalence in 80-84 years of age • >40% prevalence in 85+ years of age • No known CVD • Women 85+ have 40% prevalence Newman AB. Circulation 1993; 88:837-845
PAD and morbidity , mortality • Affects 8 million people in USA • $21 billion dollars/year- hospitalizations, meds¹ • Associated with CAD, CVA • 2-3 x increase in all cause and CV-related mortality • PAD risk factors less likely to be treated aggressively if no other atherosclerosis • Associated with poorer function- affects ADLs, Quality of Life ( McDermott 2001) • 5 years: worsening symptoms, 5% amputation
Risk Factors PAD • Tobacco abuse • Diabetes mellitus • Hyperlipidemia • Hypertension • Age over 40 • Atherosclerosis of other vessels • Known chronic kidney disease, AA, organ transplant recipients
Tobacco in PAD • Tobacco use increases risk of PAD 9 fold • Estimated 90% PAD pts smoke or have smoked cigarettes • Decrease prostacyclin • Reduction of smoking slows progression to critical leg ischemia, risks for MI • ? Effect on claudication
DM in PAD • Increases risk up to 17 fold • 28% increase in risk PAD for each 1% HgA1c elevation¹ • PARTNERS study² • ABI screening in close to 7,00 pts either over 70 or 50-69 and + tob or + DM • Prevalence of PAD 29% • Asymptomatic PAD 13% ( usually atypical symptoms) • Direct nerve damage, inflammation, endovascular damage ¹UKPDS 59 ²Hirsch AT et al JAMA 2001
Total cholesterol increased in PAD ( CV Health Study) Increased claudication in graded treadmill test Lower HDL associated with claudication in men Higher TC, LDL associated with claudication in women Hyperlipidemia in PAD
HTN in PAD • 50-92% of PAD patients have HTN • 2.5-4x increase risk of developing PAD for men/women with HTN
Clinical Diagnosis of PAD • Claudicare= limp, in Latin • Intermittent claudication (IC) prevalence 2-5%, increases with age. • 33% in one study (referral bias)¹ • Pain, cramp, fatigue over affected lower limb ( 10-30% dx with ABI have classic sx) • Atypical symptoms (48%) • No symptoms( 20%) 1. McDermott M Ann Int Med 2002;136:873-883.
Localizing vessel damage by localization of pain • Aortoiliac buttock/hip • S. Fem art upper 2/3 calf • Popliteal lower 1/3 calf • Common Fem thigh, calf or both ( normal fem pulses) • Tibial/peroneal Foot
PAD clinical signs • Skin: rubor, pallor • Decreased hair (not specific) • Nail ridging • Bruits: e.g. fem bruit + LR 4.7 • Decreased pulses • Absent femoral pulse + LR 7.1, -LR 0.9 • Other atherosclerosis( e.g., eye, CV) • Tissue ulcer • gangrene
Ankle-brachial index • Ratio of systolic BP in either p. tibialis or d. pedis over brachial artery using doppler. • Sensitivity 95%, specificity 100% ; + LR 8.6 • Normal ratio 1± 0.1 • Abnormal < 0.9 or > 1.4 • Mild < 0.8 • Moderate < 0.6 • Severe < 0.4 • Any vertical ( above/below) or horizontal ( L vs. R) change of ≥ 20 mmHg is significant • Cannot be used to categorize typical IC vs. atypical leg pain
Goals of PAD Therapy • Relieve exertional symptoms • Improve walking capacity • Improve quality of life
Case 2 • 72 yo woman with hx DM type 2, peripheral neuropathy, low back pain, CAD who presents for scheduled follow up. Family states she is not as active. • What is the risk of PAD and effect on function?
PAD and decreased function • Greater mean annual decline in 6-minute walk for those with lowest baseline ABI • Decreased usual and fastest 4-meter walking velocity • Asymptomatic PAD ( vs. normal) • 7 fold increase in 6-minute walk decline in 2 years • OR 3.63 becoming unable to walk for 6 minutes continuously McDermott MM, JAMA;292:453-461.
Atypical Symptoms in PAD • Better function on six-minute walk than pts with IC • Atypical exertional leg pain/carry on • Atypical exertional leg pain /stop group • Worse function than IC patients • No Exertional leg pain/inactive ( walks ≤ six blocks/week) • Leg pain on exertion and rest • Also slower chair rises, tandem stand, slower 4-meter velocity • More likely DM, neuropathy, spinal stenosis, other McDermott MM JAMA 2001;286;1599-1606
Walking • “Stop smoking and keep walking” • Supervised, structured program the best • 3-5x per week, 35 min of intermittent walking initially then goal of 50 minutes each • Treadmill or track best • Set grade/speed on treadmill to elicit IC sx in 3- 5 minutes • Rest until sx resolve • Resume until goal time achieved • Modify speed/grade as IC symptoms improve over time • Increased walking time by an average of 150% • Improved QOL ( self-reported physical activity, ADLs) • Reduces atherosclerosis and prothrombotic factors • Effects on amputations unknown Stewart KJ et al. NEJM 2002;347:1941-1951
Cilostazol for PAD • Phospodiesterase type 3 inhibitor→↑cAMP • Platelet aggregation inhibitor • prevents thrombi and vascular smooth muscle formation • promotes vasodilatation • Increased total distance walked ( by 50%), pain-free walking • Improved function, QoL, SPF 36 • Better than pentoxifylline • No effect on CV mortality, CV events • 50-100 mg po BID • CP450, reduce dose if on diltiazem, erythromycin, ketoconazole
Pentoxifylline for PAD • Methylxanthine derivative • Improves RBC deformability ( rheology) • Decreases fibrinogen • Antiplatelet effect • Side effect: nausea • Improvement in walking distance not as significant as cilostazol • Small studies • Reserve for non-intervention, non-cilostazol candidates, short therapy 2- 3 months • 400 mg po TID
Reduction of risk factors in PAD • Tobacco • ASA • DM • No direct effect on PAD • HTN • ACEI increased perfusion, distance walked, cardioprotective (HOPE) using ramipril • B-blockers not contraindicated; may use ISA, if needed • Lipids • Simvastatin reduced cardiovascular events 36% vs. placebo ( HPS) • Therapy improves endothelial function, decreases femoral atherosclerosis • General CV risk reduction
References • Mahoney EM et al. One year costs associated with vascular hospitalizations and chronic medication use with or at risk for atherothrombosis in the United States. Circulation-Cardiovascular Health and Outcomes 2008; 1:38-45 • McDermott MM, Greenland P, Liu K et al. Leg Symptoms in Peripheral artery Disease. JAMA 2001;286:1599-1606. • Newman AB, Siscovik DS, Manolio TA, et al. Ankle-arm index as a marker of atherosclerosis in the Cardiovascular Health Study. Circulation 1993; 88:837-845. • Hirsch AT, Criqui MH, Treat-Jacobson D, et al. Peripheral arterial disease detection, awareness and treatment in primary care. JAMA 2001;286:1317-1324. • McDermott MM, Greenland P, Liu K, et al. The Ankle Brachial Index is associated with Leg Function and Physical Activity: The Walking and Leg Circulation Study. Ann Int Med 2002; 136:873-883. • McDermott MM, Liu K, Greenland P et al. Functional Decline in Peripheral Artery Disease. JAMA 2004;292:453-461. • Hiatt WR. Medical treatment of peripheral arterial disease and claudication. NEJM 2001;344:1608-21. • Stewart KJ, Hiatt WR, Regensteiner JG, Hirsch AT. Exercise Training for Claudication. NEJM 2002; 347:1941-1951.
References 2 • Robless P, Mikhailidis DP, Stansby GP. Cilostazol for peripheral arterial disease. Cochrane Database of Systematic Reviews 2008; 1:1- • Olin JW, Sealove BA. Peripheral Artery Disease: Current Insight into the Disease and Its Diagnosis and Management. Mayo Clin Proc. 2010;85(7):678-692. • Adler AI, Stevens RJ, Neil A et al. UKPDS 59: Hyperglycemia and other potentially modifiable risk factors for peripheral vascular disease in type 2 diabetes mellitus. Diabetes Care 2002; 25:894-899.